Patients undergoing glaucoma filtration surgery often have high expectations for their postoperative visual outcomes. Glaucoma surgeons—many of whom enjoy the results of the refractive cataract procedures they perform—recognize and are frustrated by patients’ slow recovery and sometimes unexpected visual results after trabeculectomy or aqueous shunt surgery. With a better understanding of the influences on postoperative recovery in challenging cases of advanced glaucoma, surgeons can adjust their plans and techniques to improve visual outcomes.
COMBINED SURGERY
Although the target IOP is ophthalmologists’ primary focus when planning glaucoma filtration surgery, it is critical that they also assess the presurgical refractive status of both the operative and the fellow eye, because cataract status and refractive error contribute greatly to the surgical plan. For example, combined phacotrabeculectomy may not be an optimal choice for patients with high myopia or hyperopia who have no immediate plans to undergo surgery on the fellow eye, especially if the existing cataract in the operative eye is relatively mild. Performing a combined procedure on these eyes entails making a refractive plan that will affect the fellow eye, because either planned emmetropia demands earlier surgery on the fellow eye to avoid anisometropia, or the patient is left pseudophakic with a high refractive error in order to match the visual acuity of the fellow eye.
On the other hand, a moderate cataract is likely to progress rapidly in eyes undergoing filtration surgery alone, and phacoemulsification performed sequentially after a trabeculectomy is well known to compromise bleb function and requires an additional trip to the OR. Most eyes with a moderate existing cataract and a need for filtration surgery will be best served by a combined procedure. In my experience, IOP results in modern combined phacotrabeculectomy and phacoemulsification-aqueous shunt surgery are identical or superior to outcomes with trabeculectomy first.
It is also worth noting that the targeted postoperative IOP will affect IOL selection in combined surgery. As the IOP decreases, so does the axial length.1,2 Selecting an IOL for a slightly myopic goal using preoperative biometry can help avoid the small hyperopic surprise that may occur when filtration surgery significantly reduces the IOP.
An exception in the planning of combined surgery for patients with a visually significant cataract may be those with high astigmatism. Such individuals deserve special consideration for toric IOLs. Sequential trabeculectomy followed by phacoemulsification with a toric lens at a later time will allow for adjustments related to any astigmatism induced by the initial trabeculectomy (to be discussed further in this article). Although a plan for sequential surgery slows postoperative recovery, the visual results will likely be more satisfactory.
RISKS OF PHACOEMULSIFICATION AFTER TRABECULECTOMY
As mentioned earlier, phacoemulsification surgery can compromise bleb function.3 On average, the IOP can rise 3 to 5 mm Hg postoperatively, which may be tolerable if the target IOP is still attainable.
Preoperative clues may foreshadow severe compromise of the bleb and IOP, however, once phacoemulsification is performed sequentially:
• The interval between trabeculectomy and phacoemulsification is short.
• The patient is already back on glaucoma medications.
• The bleb’s appearance is low, fibrotic, or localized.
• Bleb-needling revisions were required after the initial surgery.
Surgeons should thoroughly explain to patients that the trabeculectomy may fail after phacoemulsification and, in patients with the characteristics just described, consider combining phacoemulsification with a bleb revision and an antimetabolite. With a sequential approach, he or she should closely monitor the bleb postoperatively and typically prescribe more frequent dosing or a longer course of steroids and antimetabolites to maintain the bleb.
EXPECTED VISUAL RECOVERY AFTER FILTRATION SURGERY
Ophthalmologists should be able to effectively counsel patients with advanced glaucoma on their expected visual recovery after filtration surgery. Slow visual recovery after trabeculectomy is the norm (median = 1 month). Recovery often takes up to 3 months, however, and may be even longer in patients with advanced glaucoma.4 A recent study of patients undergoing surgery with the Ex-Press Glaucoma Filtration Device (Alcon) showed an earlier visual recovery at 1 month compared to 3 months in the trabeculectomy group.5
Slow visual recovery is likely related to many factors, but one is induced astigmatism.6 Most studies find that the superior cornea flattens in the axis of the trabeculectomy site, causing early with-the-rule astigmatism. This effect is more pronounced in eyes that have a low IOP. During the first 3 months, the with-the-rule astigmatism will relax, and some patients may even develop against-the-rule astigmatism over longer periods of time.
TECHNICAL ADJUSTMENTS TO IMPROVE REFRACTIVE OUTCOMES
Some trabeculectomy techniques that I have found to effectively minimize surgically induced astigmatism include the use of gentle cautery and narrow scleral flap dissection at the 12-o’clock position to avoid the oblique axis for any induced cylinder. (To see Dr. Mattox demonstrate this technique, watch the video at http://eyetube.net/?v=inora.) In addition, I use a crescent blade to create a scleral tunnel far into the anterior clear cornea. I then convert it to a partial scleral flap by cutting radially towards the limbus but stop short of the “limbal ring.” The punch sclerostomy is small and far anterior in the cornea.
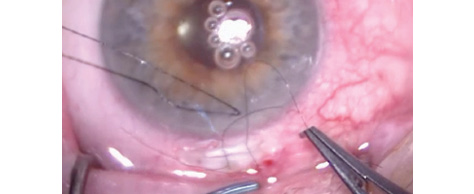
Figure. A narrow scleral tunnel converted to a partial flap, with two 10–0 nylon sutures evenly tensioned. The conjunctiva will be closed using a polyglactin suture and the Condon closure technique to further distribute the forces across the superior limbus.
In my experience, these techniques preserve the integrity of the more rigid limbal area to minimize against-the-rule relaxation. I also tie the two scleral flap sutures evenly and use a polyglactin suture and Condon closure of the conjunctiva that then relaxes, as the suture softens, to distribute forces more evenly across the superior limbus (Figure).
Eyes that receive an aqueous shunt may develop diplopia. Fortunately, this complication occurs infrequently (about 5% of eyes7), and it is typically managed effectively with spectacle prism correction. Gentle intraoperative handling of the rectus muscles or cautery near them and an avoidance of large, tense, encapsulated blebs over the shunt plates should help to minimize the development of disabling diplopia.
CONCLUSION
Visual outcomes after trabeculectomy and aqueous shunt surgery are important but sometimes overlooked in ophthalmologists’ quest to lower IOP. Their attention to patients’ preoperative refractive status and adjustment of the surgical plan or technique will help to optimize visual outcomes. n
Cynthia Mattox, MD, is an associate professor and vice chair, Department of Ophthalmology, Tufts University School of Medicine, New England Eye Center, Boston. She acknowledged no financial interest in the product or company mentioned herein. Dr. Mattox may be reached at (617) 636-8108; cmattox@tuftsmedicalcenter.org.
1. Law SK, Mansury AM, Vasudev D, Caprioli J. Effects of combined cataract surgery and trabeculectomy with mitomycin C on ocular dimensions. Br J Ophthalmol. 2005;89:1021-1025.
2. Saeedi O, Pillar A, Jefferys J, et al. Change in choroidal thickness and axial length with change in intraocular pressure after trabeculectomy. Br J Ophthalmol. 2014;98: 976-979.
3. Nguyen DQ, Niyadurupola N, Tapp RJ, et al. Effect of phacoemulsification on trabeculectomy function. Clin Experiment Ophthalmol. 2014;42(5):433-439.
4. Francis BA, Hong B, Winarko J, et al. Vision loss and recovery after trabeculectomy, risk and associated risk factors. Arch Ophthalmol. 2011;129(8):1011-1017.
5. Netland PA, Sarkisian SR, Moster MR, et al. Randomized, prospective, comparative trial of Ex-Press Glaucoma Filtration Device versus trabeculectomy (XVT Study). Am J Ophthalmol. 2014;157:433-440.
6. El-Saied HMA, Foad PH, MD, Eldaly MA, Abdelhakim MASE. Surgically induced astigmatism following glaucoma surgery in Egyptian patients. J Glaucoma. 2014;23:190-193.
7. Rauscher FM, Gedde SJ, Schiffman JC, et al, on behalf of the Tube Versus Trabeculectomy Study Group. Motility disturbances in the Tube Versus Trabeculectomy Study during the first year of follow-up. Am J Ophthalmol. 2009;147:458-466.