

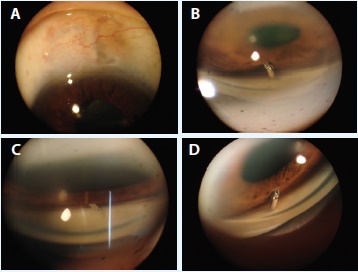
Figure 1. A preoperative external photograph of the bleb in the right eye. The bleb appears diffuse and elevated with healthylooking conjunctiva (A). Gonioscopic photographs of the right eye demonstrate the malpositioned Ex-Press shunt embedded in the iris stroma before (B) and after (C) pupillary dilation. A preoperative gonioscopic photograph of the patient’s left eye demonstrates a properly positioned shunt (D).
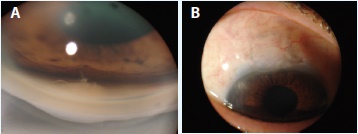
Figure 2. A gonioscopic photograph shows the postoperative appearance of the angle. The sclerostomy is patent, and the iris stroma is indented, marking the former location of the shunt (A). A postoperative external photograph of the bleb (B).
CASE PRESENTATION
A 71-year-old woman with an unremarkable general medical history and an ocular history of primary open-angle glaucoma underwent bilateral placement of an Ex-Press Glaucoma Filtration Device (Alcon) in 2011. The surgery was performed by a glaucoma specialist. After several visits with her initial surgeon, the patient presented to our practice 6 months postoperatively for a second opinion. She complained of extreme pain in her right eye but stated she felt no pain in her left eye. The patient reported that the pain in her right eye began the day after surgery. The postoperative course in her left eye, which was operated on first, had been unremarkable.
Upon examination, the patient’s BCVA was 20/25 OU, and her IOP measured 10 mm Hg in both eyes with Goldmann applanation. Low, diffuse, healthy-appearing blebs were noted in both eyes (Figure 1A). The patient was not taking ocular medication. A slit-lamp examination of the right eye showed that the internal tip of the shunt was embedded in the iris stroma. A careful gonioscopic examination confirmed this finding (Figure 1B and 1C). Movement of the iris caused a deep groove in the iris stroma from contact with the shunt (apparent only after shunt removal; Figure 2A).
The patient also had cataracts that were not visually significant. Trace anterior chamber inflammation was seen in the right eye but not in the left. After an unsuccessful 3-week trial of cycloplegic treatment (atropine sulfate ophthalmic solution 1% twice daily), topical ketorolac tromethamine ophthalmic solution, and prednisolone acetate 1%, we concluded that the patient’s eye pain was probably caused by the shunt’s touching a sensory nerve in the iris stroma.1 Given the healthy-appearing blebs, we were extremely reluctant to remove the shunt using the approaches previously described in the literature, such as taking down the conjunctiva and lifting the flap via an ab externo approach.2
Watch It Now
Watch Drs. Fellman and Grover deliver the Ex-Press device into the anterior chamber and remove it through a corneal paracentesis.
HOW WOULD YOU PROCEED
• Would you remove the shunt, take down the conjunctiva, and revise the trabeculectomy?
• Would you remove the shunt, close the scleral flap entirely, and perform a second adjacent trabeculectomy/Ex-Press device implantation?
• Would you remove the shunt, close down the trabeculectomy site, and place a glaucoma drainage implant?
• Would you perform a peripheral laser iridotomy and hope that the shunt did not become blocked by iris debris?
• Would you do nothing?
SURGICAL COURSE
We were concerned that the bleb would eventually fail if we violated the conjunctiva, and we did not want to place a tube shunt or perform a second trabeculectomy. We were also concerned that iris debris would block the 50-µm lumen of the Ex-Press device if we performed an iridectomy. We therefore developed a minimally invasive ab interno method to remove the device.
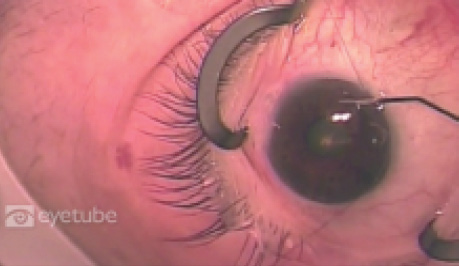
Using an ab interno approach, we visualized the angle indirectly through a four-mirror gonioprism and carefully dissected around the tip of the shunt with a 23-gauge microvitreoretinal (MVR) blade. After sufficient dissection, we delivered the shunt into the anterior chamber and removed it through a corneal paracentesis. We then used microsurgical scissors to enlarge the sclerostomy. Although it was not performed in this case, we feel surgeons should perform an ab interno iridectomy to prevent the iris from blocking the sclerostomy site, and now we routinely do so. This technique was initially described by Grover et al in 2011.3 If the Ex-Press site is located slightly nasally, a direct approach for removal may be possible with a Swann-Jacob type of goniolens.

Figure 3. Overview of the procedure. Scleral tissue adjacent to the shunt is incised with a 25-gauge MVR blade (A). The lumen of the shunt is cannulated with the MVR blade (B). The distal tip of the shunt is directed posteriorly, allowing the anterior lip to be delivered into the anterior chamber (C, D). Microsurgical forceps are used to retrieve the shunt and remove it from the anterior chamber through the corneal incisions (E,F).
OUTCOME
After ab interno removal of the malpositioned shunt, the patient’s pain immediately and completely resolved, and she was pain free on postoperative day 1. She was treated with antibiotic drops for 1 week and topical steroid drops for 2 months.
Since her operation over 3 years ago, there has been no morphologic change in the bleb in her right eye (Figure 2B) and no change in the IOP.
At the 12-month postoperative visit, the patient’s visual acuity was 20/25 OU, she had no anterior chamber inflammation, her IOP was 12 mm Hg in both eyes, her blebs appeared healthy, and she was taking no ocular medication. Figure 2 illustrates the postoperative gonioscopic findings. We would like to note the persistent defect and depression in the iris stroma.
At postoperative month 24, the patient underwent cataract surgery in both eyes. Her cataracts were not significantly worse in one eye compared with the other. We do not feel the ab interno removal of the Ex-Press causes clinically significant cataract progression.
DISCUSSION
The implantation of an Ex-Press device has increased in popularity as a glaucoma surgical procedure. There will therefore naturally be a concomitant increase in complications associated with this implant. The shunt can be malpositioned, blocked by intraocular debris, or eroded.4-6 Disturbing the conjunctival bleb associated with a shunt can lead to bleb failure and possibly to additional invasive glaucoma procedures.
Over the past 3 years, we have been using the novel ab interno approach for removing the Ex-Press shunt described herein, and we find it clearly offers many advantages over an external approach (Figure 3). We have not experienced any complications in the 25 to 30 cases we have performed. We now routinely perform ab interno iridectomies in patients with relatively floppy irides, because we have seen the iris occlude the sclerostomy.
In addition to sparing the conjunctiva, ab interno removal is more efficient and less traumatic than an external approach. Surgeons who are proficient in gonioscopy-assisted angle surgery should not have difficulty with this approach. We also now understand that the internal malpositioning of the Ex-Press shunt may cause debilitating chronic eye pain when the steel tube is deeply embedded in the iris, especially in phakic patients in whom the iris tends to vault forward. The ability to remove the shunt via an atraumatic ab interno approach is especially useful when the device is internally malpositioned in an eye with a functioning bleb.
More importantly, we have also found the technique useful for removing the device when the bleb has failed and the surgeon takes the patient back to the OR for subsequent incisional glaucoma surgery. It seems reasonable to remove a nonfunctioning intraocular metallic foreign body, because it serves no purpose. When doing so is possible and safe, we remove shunts that have failed if the patient requires an additional operation. Although the Ex-Press device has been shown to be safe with a low likelihood of erosion,2,4-6 long-term data on its safety for 10 to 15 years are not yet available. If necessary, the minimally invasive approach we described can be used to safely remove shunts at high risk of erosion.
Thankfully, our patient has done extremely well, and we have over 3 years of follow-up data. She, along with thousands of others, continues to demonstrate that patients are doctors’ best teachers and force physicians to improve and innovate to optimize the care they provide. n
1. The eye. In: Cibis GW, Beaver HA, Johns K, et al, eds. Fundamentals and Principles of Ophthalmology. San Francisco, CA: American Academy of Ophthalmology; 2006; 418-419. American Academy of Ophthalmology Basic and Clinical Science Course: 2006-2007; section 2.
2. Stein JD, Herndon LW, Brent Bond J, Challa P. Exposure of Ex-Press miniature glaucoma devices: case series and technique for tube shunt removal. J Glaucoma. 2007;16(8):704-706.
3. Grover DS, Fellman MA, Fellman RL. New ab interno technique for removal of iris-embedded Ex-Press shunt and chronic eye pain caused by shunt malpositioning. JAMA Ophthalmol. 2013;131(10):1356-1358.
4. Stewart RM, Diamond JG, Ashmore ED, Ayyala RS. Complications following Ex-Press glaucoma shunt implantation. Am J Ophthalmol. 2005;140(2):340-341.
5. Garg SJ, Kanitkar K, Weichel E, Fischer D. Trauma-induced extrusion of an Ex-Press glaucoma shunt presenting as an intraocular foreign body. Arch Ophthalmol. 2005;123(9):1270-1272.
6. Tavolato M, Babighian S, Galan A. Spontaneous extrusion of a stainless steel glaucoma drainage implant (Ex-Press). Eur J Ophthalmol. 2006;16(5):753-755.
Ronald L. Fellman, MD
• glaucoma specialist, Glaucoma Associates of Texas, Dallas
• clinical associate professor emeritus, Department of Ophthalmology, UT Southwestern Medical Center, Dallas
• (214) 360-0000; rfellman@glaucomaassociates.com
• financial interest: none acknowledged
Davinder S. Grover, MD, MPH
• glaucoma specialist, Glaucoma Associates of Texas, Dallas
• clinical instructor, Department of Ophthalmology, UT Southwestern Medical Center, Dallas
• dgrover@glaucomaassociates.com
• financial interest: none acknowledged