

CASE PRESENTATION
A 15-year-old boy with a history of cryotherapy-treated retinopathy of prematurity (ROP) in the right eye was referred by his pediatrician to a community ophthalmologist for conjunctivitis. The patient said he had experienced no eye pain or change in vision. The IOP in his right eye measured 38 mm Hg, and there was an afferent pupillary defect. Gonioscopy revealed a trace cell in the anterior chamber and appositional angle closure. The IOP was within normal limits in the patient’s left eye. He was treated with topical brinzolamide, brimonidine, timolol, and difluprednate.
AT A GLANCE
• The success rate of trabeculectomy in children is lower than in adults.
• Children may have up to a 32% rate of tube migration requiring surgical intervention.
• Compared to adults, children also have a higher risk of endophthalmitis, whether they are undergoing trab- eculectomy or GDD implantation, but the risk is much lower for a GDD.
Upon follow-up the next day, the patient’s IOP was 10 mm Hg, and a laser peripheral iridotomy was performed. The IOP normalized initially but increased to 38 mm Hg 2 weeks later. The patient was referred to the Glaucoma Service at the Flaum Eye Institute at the University of Rochester in November 2014 for possible surgical management.
Upon presentation, the patient’s visual acuity was 20/50 OD and 20/25 OS. There was an afferent pupillary defect in the right eye, and IOP by applanation tonometry measured 44 mm Hg OD and 15 mm Hg OS. An examination of the anterior segment of the right eye showed a clear cornea, a patent iridotomy, a quiet anterior chamber, a clear lens, and a combination of appositional and synechial angle closure on gonioscopy. The right disc appeared to slope superiorly, and the left disc appeared crowded.
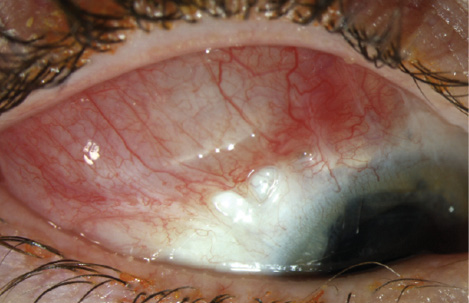
Figure 1. An examination in April 2015 showed the plate beginning to migrate anteriorly and the tube still in place in the anterior chamber (arrow).
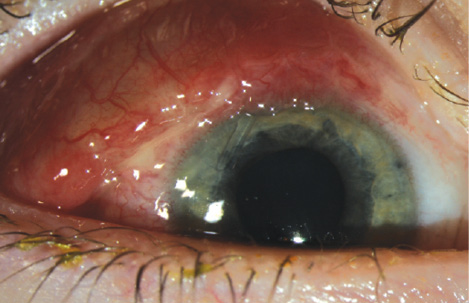
Figure 2. An examination in June 2015 demonstrated further anterior migration of the plate. The tube remained in the anterior chamber (arrow).
We proceeded with urgent surgery and implanted an Ahmed Glaucoma Valve (model FP7; New World Medical) with a scleral patch graft in the superotemporal quadrant of the right eye. We used 9–0 nylon sutures to secure the plate to the sclera. Initially, the patient did well on no glaucoma medications. His IOP measured between 6 and 13 mm Hg for the first 5 months postoperatively. In April 2015, the plate was noted to be anteriorly displaced (Figure 1). The patient had recently started karate lessons but denied any direct trauma to the right eye. The IOP was still well controlled at 5 mm Hg, and he was asked to avoid contact sports.
At the follow-up examination in June 2015, the plate had become further displaced anteriorly, with the long axis lying along the limbus (Figure 2). The IOP measured 5 mm Hg.
We scheduled the patient for surgery to reposition the plate. On the day of the surgery, however, the conjunctiva was found to have dehisced, and the plate had completely extruded in the preoperative holding area. The plate was surrounded by significant mucopurulent discharge, and the tube was still evident in the anterior chamber (Figure 3). The patient’s father stated that the dehiscence had occurred a few days earlier.
HOW WOULD YOU PROCEED?
- Would you explant the plate and replace it with a new tube shunt on the same day?
- Would you explant the plate and replace it with a new tube shunt via a staged approach?
SURGICAL COURSE
Before prepping the surgical field with povidone-iodine, we swabbed the plate and surrounding discharge for aerobic, anaerobic, fungal, and acid-fast bacilli cultures. We then prepped and draped the patient’s eye in a sterile fashion. Under the operating microscope, it was evident that only the temporal suture was still intact, securing the plate to the sclera 8 mm posterior to the limbus. We noted no hypopyon or hyphema within the anterior chamber.

Figure 3. On the date of the planned repositioning of the plate, the conjunctiva had dehisced, with total anterior migration and exposure of the glaucoma drainage device (GDD) plate. Significant mucopurulent discharge was noted.
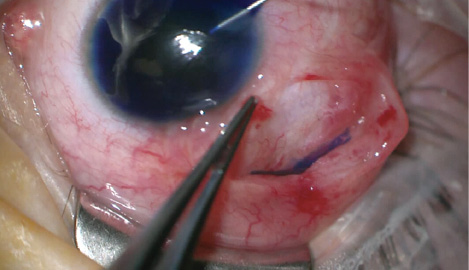
Figure 4. The surgeons injected trypan blue ophthalmic solution into the anterior chamber, and the dye pooled 6 to 7 mm posterior to the limbus, where the overlying plate had caused a localized area of scleral erosion.
We cut the intact suture and explanted the shunt in toto. After making a paracentesis, we injected carbachol to reform the anterior chamber and constrict the pupil. We injected additional balanced salt solution, but the anterior chamber continued to collapse. Fluid pooled approximately 6 to 7 mm behind the limbus, at the former location of the dehisced nasal suture. We injected trypan blue ophthalmic solution intracamerally to localize the site of leakage. Pooling of the dye occurred at the same location, suggesting the presence of a scleral-anterior chamber fistula at this site (Figure 4), presumably due to scleral thinning from prior cryotherapy (to be discussed further). The sclera in this area was very thin and spongy, and initially, the sutures “cheesewired” through the tissue with attempted closure. Ultimately, we placed a 10–0 nylon suture (Ethicon) to close the leak.
We irrigated the exposed scleral surface with cefazolin for endophthalmitis prophylaxis. The edges of the conjunctiva were then closed with a 9–0 Vicryl suture (Ethicon). We deepened the anterior chamber with Healon (Abbott Medical Optics) to avoid postoperative hypotony.
OUTCOME
We prescribed a standard postoperative course of topical antibiotic and steroid drops. The cultures taken from the plate were all negative. The bacterial cultures of the discharge were positive for three colonies of Corynebacterium and one colony of coagulase-negative Staphylococcus.
On the first postoperative day, the IOP measured 8 mm Hg, but it rose to 35 mm Hg after the first week. The patient was restarted on topical brimonidine-brinzolamide and bimatoprost. On the next visit 1 week later, his IOP was well controlled at 18 mm Hg. The patient did not develop endophthalmitis.
DISCUSSION
This case raises several issues regarding the choice of surgical technique as well as implications for surgery on eyes with a history of ROP.
We initially chose a GDD rather than a trabeculectomy to maximize the probability of surgical success in this young patient (Table). The success rate of trabeculectomy in children is lower than in adults (35%-50% vs 50%-90%).1-3 Children demonstrate more exuberant bleb encapsulation postoperatively, precluding suture lysis and increasing the risk of surgical failure.4
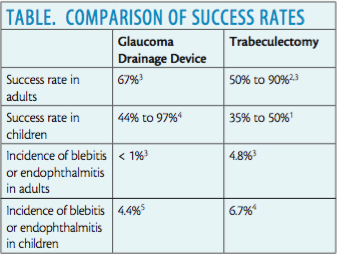
Whether they are undergoing trabeculectomy or the implantation of a GDD, children have a higher risk of endophthalmitis than adults, but the risk is much lower for a GDD. The incidence of endophthalmitis or blebitis after trabeculectomy in children is 6.7%5 compared with 4.8% in adults.3 In contrast, the incidence of endophthalmitis or blebitis after GDD implantation in children is 4.4%,6 whereas it is less than 1% in adults.3
Nonetheless, the index of clinical suspicion of infection associated with a GDD in children must be high. Major risk factors include conjunctival erosion and tube exposure, with a 13% incidence of the latter.7 Given these risks and the presence of mucopurulent discharge, we decided to remove the potential source of infection by explanting the tube shunt, with a plan to control IOP medically and closely monitor the child postoperatively for the development of endophthalmitis. Fortunately, despite extrusion of the GDD and significant mucopurulent discharge, the inflammation was largely sterile on culture and did not lead to endophthalmitis in this patient.
A 1.4% incidence of Ahmed Glaucoma Valve extrusion in adults has been reported,8 and children may have up to a 32% rate of tube migration requiring surgical intervention.4 At our practice, tube migration has been a rare occurrence. We believe it likely that the patient had an abnormally thin sclera due to his history of ROP, leading to this late-onset surgical complication.
The sclera is more thin and fragile in eyes with ROP than in healthy eyes, and the tissue may become even more friable after treatment with cryotherapy. Erosion of the sclera after scleral buckling in an eye with cryotherapy-treated ROP has been reported.9 A similar mechanism may have occurred in this case, with dehiscence of the nasal nylon suture securing the plate and weakening of the already-thin sclera at the suture site. Presumed trauma from contact sports may have loosened the suture; alternatively, normal ocular excursions could have caused the GDD to shift10 and thus weakened the suture.
To date, the patient’s IOP has been well controlled on topical therapy for 4 months after removal of the Ahmed Glaucoma Valve, with the IOP ranging between 18 and 25 mm Hg. If the patient requires repeat surgical intervention in the future, special care will be needed to avoid repeat scleral erosion. If an area that has not undergone prior cryotherapy can be identified, a repeat GDD could be attempted in a different quadrant. The use of a thicker suture such as 8–0 nylon and a deeper scleral bite might also affix the plate more securely. As the patient ages and the risk of endophthalmitis decreases, a trabeculectomy may also become a viable option. Finally, as the options for angle surgery expand, an ab interno angle procedure in the areas of appositional angle closure combined with cataract surgery may be beneficial to this patient. n
The authors would like to thank Rachel Hollar, BS, CRA, OCT-C; Brittany Richardson, COA, CRA, OCT-C; and Taylor Pannell, BS, CRA, OCT-C, for the slit-lamp photographs.
1. Scuderi G, Iacovello D, Pranno F, et al. Pediatric glaucoma: a literature’s review and analysis of surgical results. Biomed Res Int. 2015;2015:393670.
2. Costa VP, Katz LJ, Spaeth GL, et al. Primary trabeculectomy in young adults. Ophthalmology. 1993;100(7):1071-1076.
3. Gedde SJ, Herndon LW, Brandt JD, et al. Postoperative complications in the Tube Versus Trabeculectomy (TVT) study during 5 years of follow up. Am J Ophthalmol. 2012;153(5):804-814.
4. Scuderi G, Iacovello D, Pranno F, et al. Pediatric glaucoma: a literature’s review and analysis of surgical results. Biomed Res Int. 2015;2015:393670.
5. Chen TC, Chen PP, Francis BA, et al. Pediatric glaucoma surgery: a report by the American Academy of Ophthalmology. Ophthalmology. 2014;121(11):2107-2115.
6. Al-Torbak AA, Al-Shahwan S, Al-Jadaan I, et al. Endophthalmitis associated with the Ahmed Glaucoma Valve implant. Br J Ophthalmol. 2005;89(4):454-458.
7. Wentzloff JN, Crosskreutz CL, Pasquale LR, et al. Endophthalmitis after glaucoma drainage implant surgery. Int Ophthalmol Clin. 2007;47(2):109-115.
8. Chen H, Zhang SX, Liu L, et al. Intermediate-term and long-term clinical evaluation of the Ahmed Glaucoma Valve implantation [in Chinese]. Zhonghua Yan Ke Za Zhi. 2005;41(9):796-802.
9. Yu YS, Chang BL. Scleral perforation after scleral buckling surgery for retinopathy of prematurity. Korean J Ophthalmol. 1999;13(1):49-51.
10. Law SK, Coleman AL, Caprioli J. Dynamic tube movement of the Ahmed Glaucoma Valve. J Glaucoma. 2009;18(8):628-631.
Katherine Fallano, MD
• resident, Flaum Eye Institute, University of Rochester School of Medicine and Dentistry, Rochester, New York
• kfallano@gmail.com
• financial interest: none acknowledged
Shakeel Shareef, MD
• associate professor, Flaum Eye Institute, University of Rochester School of Medicine and Dentistry, Rochester, New York
• (585) 273-3937; shakeel_shareef@urmc.rochester.edu
• financial interest: none acknowledged