
Visual field testing is paramount in diagnosing and observing patients with glaucoma, and advances such as better testing algorithms, fixation strategies, and reliability indices, as well as shorter test duration and new progression analyses, have improved clinicians’ ability to detect changes. The value of these improvements, however, ultimately depends on the patient’s ability to take the test, the technician’s skill at administering it, and the physician’s interpretation. By taking steps to address these subjective elements, you can increase the value and reliability of visual fields.
AT A GLANCE
• Advances have made visual field tests shorter and more accurate.
• Patient, technician, and physician factors can still limit the value of visual fields.
• An optimized test for a specific patient performed in the best possible manner with the least time wasted is essential for the best results.
INDIVIDUALIZE CHOICES
Most patients do not like visual field tests, so it is important to select the optimal test parameters to gain the most information in the shortest time. A suboptimal test choice in a patient with vision loss could lead to poor reliability during testing and unreliable fields. Set the patient up to succeed by selecting the best test algorithm, test object size, and field area for his or her stage of disease. Remember that the optimal test for diagnosing disease may not necessarily be the same when monitoring glaucoma. For example, short-wavelength automated perimetry can show visual field abnormalities in patients at high risk of developing glaucoma even when white-on-white visual fields are within normal limits. Be specific about the area that needs testing. Use 10-2 visual fields instead of 24-2 or higher if the field is severely constricted (Figures 1 and 2).

Figure 1. A 24-2 visual field: central 24° of field tested.
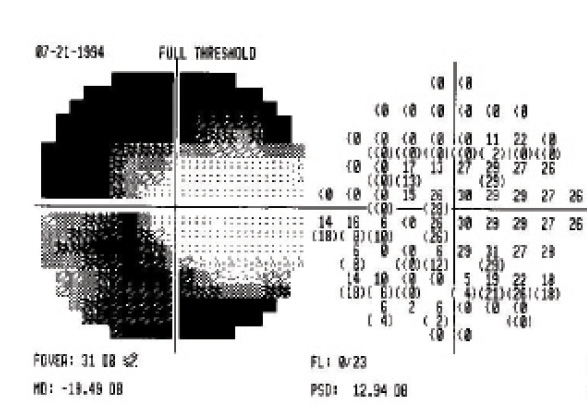
Figure 2. A 10-2 visual field: central 10° of field tested.
KEEP PATIENTS COMFORTABLE
Patients need a quiet test environment where they can comfortably hold one position for 20 to 30 minutes. If the patient cannot tolerate the full-length test, change the algorithms to shorten the test time. If a field is dire, consider using the Swedish Interactive Threshold Algorithm instead of the full threshold and Swedish Interactive Threshold Algorithm Fast in young and elderly patients if a field is dire. Take advantage of progression analysis; use StatPac on the Humphrey Field Analyzer (Carl Zeiss Meditec) to monitor field indices and reliability. If repeated tests are low yielding, follow progression with other tests.
Watch it Now
Chris Johnson, PhD, discusses techniques for tracking visual field progression.

Even simple fatigue and discomfort on the patient’s part make the visual fields appear worse. Try testing one eye at each visit, or begin with alternating eyes at each visit. If fixation losses are high, give the patient short breaks. Talk to patients about the learning curve, test spot retesting, the ability to hold down the trigger to stop the test to take a break, and the effects of blinking. It is worthwhile to advise patients to get a good night’s rest and to avoid eating right before the test.
TECHNICIAN TRAINING
A technician’s ability to put the patient at ease is priceless. Observe the testing process to identify and correct any problems that may arise. Does the technician offer encouragement or a countdown? Provide training and feedback as needed. Train technicians on in-office testing protocol, including checking current vision, confirming which tests have already been administered, switching the order of eyes tested, and communicating any issues that could affect the test results such as a patient’s falling asleep. It can also help to have staff take the test so that they know what it feels like.
IMPROVE RELIABILITY
Visual field testing does not just assess peripheral vision but also the space one eye can see in any given instance. It is important to reassure patients that there could be a learning curve and to let them know that there is test spot retesting during the visual field. This could help improve reliability during testing.
Remember that coexisting medical conditions such as Alzheimer disease, tremors, and arthritis can affect test results. Patients may be unable to take tests reliably in these scenarios, making interpretation difficult. It may be best in these instances to follow the patient’s disease with other tests.
CONCLUSION
Visual field testing is an art that works best when all the variables involved come together. Its value and reliability depend on the combined effort of physicians, technical staff, and patients. An optimized test for a specific patient performed in the best possible manner with the least time wasted is essential for the best results. n
Oluwatosin Smith, MD
• attending physician, Glaucoma Associates of Texas, Dallas
• (214) 360-0000; tsmith@glaucomaassociates.com or olutos@yahoo.com
• financial interest: none acknowledged