
Although the basic visual field test procedure of detecting a small target superimposed on a uniform background has been used for more than 2,000 years,1 there have been major advances in the standardization and optimization of testing procedures and analytical methods. Additionally, there is a growing need for the ability to perform diagnostic procedures such as perimetry in a variety of settings (waiting rooms, homes, remote clinics with limited resources, etc.) as well as for tests that provide information on the performance of tasks. This article provides a brief overview of these innovations.
AT A GLANCE
• There is a growing need for the ability to perform diagnostic procedures such as perimetry in a variety of settings and for tests that provide information on the performance of tasks.
• Investigators are developing diagnostic vision testing procedures that can be performed with smartphones and tablets. The technology provides an opportunity to make ophthalmic diagnostic tests available to individuals with limited access to traditional health care.
• Standard visual field testing is useful and important for monitoring the status of glaucoma patients, determining whether their condition is stable or progressing at a particular rate, and making treatment decisions. These procedures are less helpful for determining whether a patient is able to perform activities of daily living and how visual impairment affects his or her quality of life. Newer tests may help in this regard as clinicians and investigators learn more about the consequences of vision impairment from ocular and neurologic diseases.
NEW TEST PROCEDURES
Standard automated perimetry (white-on-white perimetry) is still the most common method of performing visual field testing in ophthalmic clinics. Many procedures have been developed, however, to test the spatial, temporal, color, and other properties of the peripheral visual field, including short-wavelength automated perimetry, frequency doubling technology and Humphrey Matrix perimetry (Carl Zeiss Meditec), Pulsar perimetry (Haag-Streit), motion perimetry, flicker perimetry, Heidelberg Edge perimetry (flicker-defined form; Heidelberg Engineering), and Rarebit perimetry.2,3 These tests provide the opportunity to evaluate specific visual functions that may be damaged earlier or more extensively than standard automated static perimetry results are able to convey. Standard automated perimetry, however, remains the most common test procedure that is used by practitioners worldwide.
As clinicians and investigators learn more about the consequences of the impairment of specific color, spatial, and temporal properties of vision by ocular and neurologic diseases, these newer tests may help to clarify the underlying basis of problems that patients encounter in terms of their quality of life and activities of daily living.
Watch it Now
Pradeep Ramulu, MD, PhD, describes how eye care providers can assess glaucoma’s impact on patients’ quality of life and use this information to provide better care.

NEW ANALYTICAL PROCEDURES
Although event analysis (change from baseline) and linear regression have been used for the analysis of visual field data and glaucomatous progression in longitudinal studies,4 more recent analytical procedures have been developed, many of them using variations of Bayesian strategies.5-10 These procedures have generated methods of enhancing the performance of visual field progression techniques that have improved sensitivity and specificity, reduced the number of tests required for a definitive analysis, and decreased the amount of time needed for an informed decision. Further refinements can be achieved by providing the analysis program with findings from an independent subset of participants or from earlier test results of the same participant that will allow the analytical method to “learn” specific patterns and sequences of visual field changes.
Additionally, there is a growing awareness of the importance of combining visual field information with other clinical results (optic disc and retinal nerve fiber layer measurements, IOP, family history, other risk factors, etc.) in order to generate a more comprehensive quantitative model of the pathologic course of glaucoma and the influence of various treatment regimens.
HOME TESTING
The technological advances evident in smartphones and tablet displays have led many investigators to develop diagnostic vision testing procedures that can be performed with these instruments.11-15 These devices have appropriate spatial and temporal properties and a suitable dynamic intensity range, they are easy to use for rapid testing, and they are quite cost-effective. The technology thus provides an opportunity to make ophthalmic diagnostic tests available to individuals with limited access to traditional health care by allowing testing to be performed in different settings (eg, waiting rooms) and making it possible for people to test themselves at home.
Figure 1. A tablet is being used for vision testing.
Because this is a relatively new approach to visual function testing, it is still in an early stage of development. Given the demands placed upon health care, particularly in underdeveloped countries and rural areas, however, interest in this area will grow rapidly in the next few years and will have a meaningful impact on the manner in which ocular and neurologic diseases are detected and monitored (Figure 1).
REAL-WORLD PRACTICAL TESTS
Standard visual field testing procedures are useful and important for monitoring the status of glaucoma patients, determining whether their condition is stable or progressing at a particular rate, and making treatment decisions. These procedures are less helpful for determining whether a patient is able to perform activities of daily living (such as driving, walking, shopping, and reading) and how visual impairment affects his or her quality of life.10,16 Tests such as the Useful Field of View (Visual Awareness Research Group)17 that incorporate attention, navigation pathways, and tests that include multitasking18 will provide greater assistance for these determinations (Figure 2).
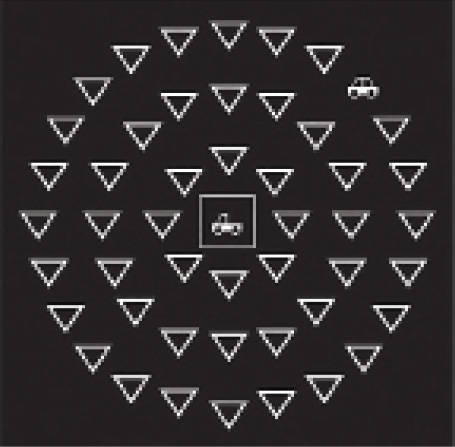

Figure 2. An example of the display presented on a computer monitor for testing the Useful Field of View.
Many subtle performance issues that have limited investigational findings (eg, hand-eye coordination18) may also lead to the development of new procedures that can be performed in the clinic.
CONCLUSION
Practitioners are entering a new era in which they will receive lower compensation for their services, clinical time with patients will be more limited, diagnostic testing will be less available in clinics, and the impact of vision impairment on daily activities will receive greater emphasis. New and different approaches to managing patients with glaucoma or at risk of developing the disease will therefore be a welcome and much-needed advance. n
1. Johnson CA, Wall M, Thompson HS. A history of perimetry and visual field testing. Optom Vis Sci. 2011;88(1):E8-15.
2. Johnson CA. Psychophysical and electrophysiological testing in glaucoma: visual fields and other functional tests. In: Choplin N, Traverso C, eds. Atlas of Glaucoma. 3rd ed. Boca Raton, FL: CRC Press; 2014:87-112.
3. Kaczorowski K, Mulak M, Szumny D, Misiuk-Hollo M. Heidelberg Edge Perimeter: the new method of perimetry. Adv Clin Exp Med. 2015;24(6):1105-1112.
4. Spry PGD, Johnson CA. Identification of progressive glaucomatous visual field loss. Surv Ophthalmol. 2002;47:158-173.
5. Russell RA, Malik R, Chauhan BC, et al. Improved estimates of visual field progression using Bayesian linear regression to integrate structural information in patients with ocular hypertension. Invest Ophthalmol Vis Sci. 2012;53:2760-2769.
6. Medeiros FA, Zangwill LM, Weinreb RN. Improved prediction of rates of visual field loss in glaucoma using empirical Bayes estimates of slopes of change. J Glaucoma. 2012;21:147-154.
7. Fujino Y, Murata H, Mayama C, Asaoka R. Applying “lasso” regression to predict future visual field progression in glaucoma patients. Invest Ophthalmol Vis Sci. 2015;56:2334-2339.
8. Zhu H, Crabb DP, Ho T, Garway-Heath DF. More accurate modeling of visual field progression in glaucoma: ANSWERS. Invest Ophthalmol Vis Sci. 2015;56(10):6077-6083.
9. Helm JE, Lavieri MS, Van Oyen MP, et al. Dynamic forecasting and control algorithms of glaucoma progression for clinician decision support. Operations Research. 2015;63:979-999.
10. Tabrett DR, Latham K. Important areas of the central binocular visual field for daily functioning in the visually impaired. Ophthalmic Physiol Opt. 2012;32(2):156-163.
11. Tahir HJ, Murray IJ, Parry NR, Aslam TM. Optimization and assessment of three touch screen tablet computers for clinical vision testing. PLoS One. 2014;9(4):e395074.
12. Kollbaum PS, Jansen ME, Kollbaum EJ, Bullimore MA. Validation of an iPad test of letter contrast sensitivity. Optom Vis Sci. 2014;91(3):291-296.
13. Wang YZ, He YG, Mitzel G, et al. Handheld shape discrimination hyperacuity test on a mobile device for remote monitoring of visual function in maculopathy. Invest Ophthalmol Vis Sci. 2013;54(8):5497-5505.
14. Chew EY, Clemons TE, Bressler SB, et al; Appendix 1 for AREDS2-HOME Study Research Group. Randomized trial of the ForeseeHome monitoring device for early detection of neovascular age-related macular degeneration. The Home Monitoring of the eye (HOME) study design – HOME Study report number 1. Contemp Clin Trials. 2014;37(2):294-300.
15. Dorr M, Lesmes LA, Lu ZL, Bex PJ. Rapid and reliable assessment of the contrast sensitivity function on an iPad. Invest Ophthalmol Vis Sci. 2013;54:7266-7273.
16. Crabb DP, Smith ND, Glen FC, et al. How does glaucoma look? Patient perception of visual field loss. Ophthalmology. 2013;120:1120-1126.
17. Ball K, Owsley C. The Useful Field of View test: a new technique for evaluating age-related decline in visual function. J Am Optom Assoc. 1993;64(1):71-79.
18. Kotecha A, O’Leary N, Melmoth D, et al. The functional consequences for eye-hand coordination. Invest Ophthalmol Vis Sci. 2009;50:203-213.
Chris A. Johnson, PhD, DSc
• professor, Department of Ophthalmology and Visual Sciences, University of Iowa Hospitals and Clinics, Iowa City, Iowa
• (319) 356-0384; chris-a-johnson@uiowa.edu
• financial disclosure: consultant to Haag-Streit and M&S Technologies