


Case Presentation
A 45-year-old woman was referred to our glaucoma practice for evaluation of narrow angles in both eyes. The patient complained of occasional pulsating brow ache but had no visual complaints. She had a history of congenital amblyopia in the left eye, for which she had been patched for many years as a child, and she had a medical history of endometriosis. Family ocular history was significant for macular degeneration. She was on no ocular or systemic medications and had no allergies.
Her BCVA was 20/20 OD and 20/30 OS with a manifest refraction of +1.00 -0.50 × 095 OD and +5.00 -1.50 × 085 OS. Her IOP, as measured by applanation tonometry, was 21 mm Hg OU, and pachymetry demonstrated central corneal thicknesses of 578 µm OD and 611 µm OS. Slit-lamp biomicroscopy was significant only for mild nuclear sclerosis in both eyes. Gonioscopy demonstrated grade 0 angles 360º bilaterally with a lumpy appearance (Figure 1). The posterior segment examination was unremarkable. Soon after the initial exam, she underwent laser peripheral iridotomy of both eyes, and the angles became grade 1.
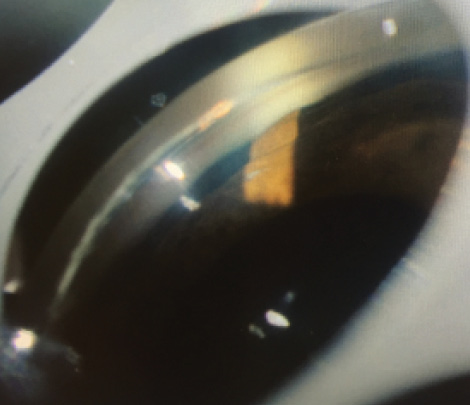
Figure 1. Gonioscopy demonstrated grade 0 angles 360º OU with a lumpy appearance in both eyes.
The patient was referred back to our practice 2 years later because of recurrent pulsating brow ache. On examination, her IOP was 22 mm Hg OD and 24 mm Hg OS. Gonioscopy demonstrated grade 0 to 1 360º bilaterally with a lumpy appearance and patent peripheral iridotomies. Optical coherence tomography (OCT) of the retinal nerve fiber layer demonstrated normal neuroretinal rim thickness in both eyes, and OCT of the macula demonstrated normal ganglion cell layer thickness as well as normal internal limiting membrane to retinal pigment epithelium thickness.
Standard automated perimetry by Swedish Interactive Thresholding Algorithm (SITA) testing demonstrated preserved field in the right eye and a cecocentral defect in the left eye. Ultrasound biomicroscopy (UBM; Figure 2) demonstrated cystic areas within and around the ciliary body, shallow anterior chambers with closed angles, and a plateau iris configuration in both eyes. Peripheral iridotomy was patent in the right eye and not visualized in the left. Anterior segment OCT (Figure 3) demonstrated closed angles consistent with gonioscopy and UBM findings.
HOW WOULD YOU PROCEED?
- Would you monitor the patient?
- Would you start pilocarpine?
- Would you perform argon laser iridoplasty?
CLINICAL COURSE
The patient underwent argon laser iridoplasty of both eyes, and her IOP remained stable in the midteens 4 months postoperatively.
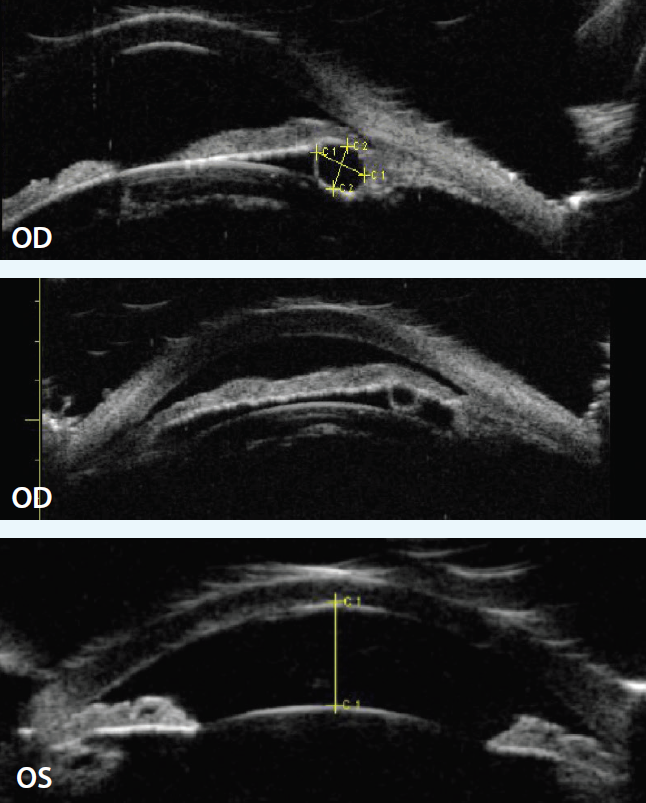
Figure 2. UBM demonstrated cystic areas within and around the ciliary body, shallow anterior chambers with closed angles, and a plateau iris configuration in both eyes.
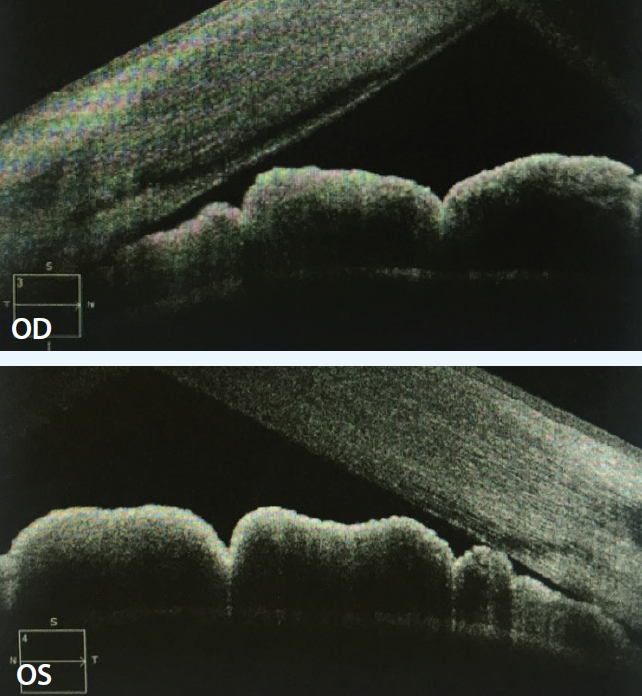
Figure 3. Anterior segment OCT demonstrated closed angles consistent with gonioscopy and UBM findings.
DISCUSSION
We present a case of ciliary body cysts creating plateau iris configuration and secondary angle-closure glaucoma (ACG), which was successfully treated with argon laser iridoplasty. In a large survey of iris tumors, 79% were solid, and 21% were cystic.1
Cystic lesions can be found in the stroma as well as iris pigment epithelium, where they are further classified as pupillary, midzonal, peripheral, or dislodged. Peripheral iris pigment epithelial cysts are one of the most common tumors, representing 14% of all iris tumors.1
Iridociliary cysts are a rare etiology for plateau iris syndrome,2 and they are characterized by a convex configuration of the peripheral iris that leads to pleateau iris configuration and a narrow angle despite the creation of a peripheral iridotomy to relieve pupillary block. Thomas et al proposed that one should have a high index of suspicion for iridociliary cysts in the setting of ACG with gonioscopic evidence of a “lumpy appearance to the angle” as well as “variability in angle width.”3
On UBM, iridociliary cysts are thin walled and have sonolucent interiors, as in our case.4,5 Given that the location of these cysts is typically at the iridociliary junction,4 a convex configuration of the angle is created, leading to plateau iris syndrome. If iridociliary cysts cover more than 180º of the iris surface,4 they can cause secondary ACG.
Additional accounts of iridociliary cysts have been found in the literature. A case report from India describes a patient with plateau iris configuration without variability in width of the angle whose IOP did not improve on pilocarpine. He was found to have iris and ciliary body cysts bilaterally. His first argon laser iridoplasty treatment session caused fluid and pigment release from cyst rupture, resulting in an IOP spike that was conservatively managed. He was successfully treated in a subsequent session.3 The management of iridociliary cysts is varied. The literature includes accounts of sector iridotomy,6 puncture of cysts, and laser treatments. The last includes iridoplasty by argon and Nd:Yag lasers.7 This case illustrates that iridoplasty is a successful treatment option for iridociliary cysts causing ACG. Its safety and efficacy will need to be validated in a larger study. n
1. Shields CL, Kancherla S, Patel J, et al. Clinical survey of 3680 iris tumors based on patient age at presentation. Ophthalmology. 2012;119:407-414.
2. Shields JA. Primary cysts of the iris. Trans Am Ophthalmol Soc.1981;79:771-809.
3. Thomas R, Mulligan N, Aylward GW, Billson FA. Angle closure glaucoma due to iris and ciliary body cysts. Aust N Z J Ophthalmol. 1989;17:317-319.
4. Marigo FA, Esaki K, Finger PT, et al. Differential diagnosis of anterior segment cysts by ultrasound biomicroscopy. Ophthalmology. 1999;106:2131-2135.
5. Crowston JG, Medeiros FA, Mosaed S, Weinreb RN. Argon laser iridoplasty in the treatment of plateau-like iris configuration as result of numerous ciliary body cysts. Am J Ophthalmol. 2005;139:381-383.
6. Naumann GO, Rummelt V. Congenital nonpigmented epithelial iris cyst removed by block-excision. Graefes Arch Clin Exp Ophthalmol. 1990;228:392-397.
7. Kuchenbecker J, Motschmann M, Schmitz K, Behrens-Baumann W. Laser iridocystotomy for bilateral acute angle-closure glaucoma secondary to iris cysts. Am J Ophthalmol. 2000;129:391-393.
Lama A. Al-Aswad, MD, MPH
•assistant professor of clinical ophthalmology at Edward S. Harkness
Eye Institute, Columbia University College of Physicians and
Surgeons, New York, New York
•(212) 305-6709; laa2003@columbia.edu
•financial interest: none acknowledged
Aakriti Garg, MD
•ophthalmology resident at Edward S. Harkness Eye Institute,
Columbia University College of Physicians and Surgeons, New
York, New York
•ag2965@cumc.columbia.edu
•financial interest: none acknowledged
James Murphy III, MD
•ophthalmologist, Fromer Eye Center, New York, New York
•(212) 832-9228; jamestmurphyiiimd@gmail.com
•financial interest: none acknowledged