CASE PRESENTATION
A 74-year-old man presents with a request for a second opinion. The patient reports experiencing progressive hazy vision that is worse in his left eye. He has a longstanding history of glaucoma that has been treated medically by another provider. The patient says he thinks something is wrong with his treatment, that the drops are making his vision worse. He complains of significant tearing and irritation. The patient is unsure what his highest IOP reading has been. His current medical regimen is a fixed combination of dorzolamide and timolol, brimonidine, and bimatoprost in both eyes. He has no history of contact lens wear and no known history of corneal infection, trachoma, or toxic chemical injury.
On examination, the patient’s visual acuity is 20/50 OD and 20/60 OS, and his IOP is 19 mm Hg OU. Central corneal thickness is 524 μm OD and 576 μm OS. A slit-lamp examination reveals conjunctival injection and a dense corneal pannus that is worse in the left eye (Figure 1). A 1+ to 2+ nuclear sclerotic cataract is present in each eye. The patient’s history is significant for bilateral laser peripheral iridotomies. Gonioscopy reveals grade 1 to 2 angles and occasional peripheral anterior synechiae (PAS). A fundus examination shows relatively healthy optic nerves and otherwise unremarkable retinas (Figure 2). OCT imaging shows a normal retinal nerve fiber layer (RNFL) in the right eye, but image capture is unreliable in the left eye (Figure 3). Humphrey visual field testing (Carl Zeiss Meditec) shows inferior changes that are more significant in the left eye (Figure 4).

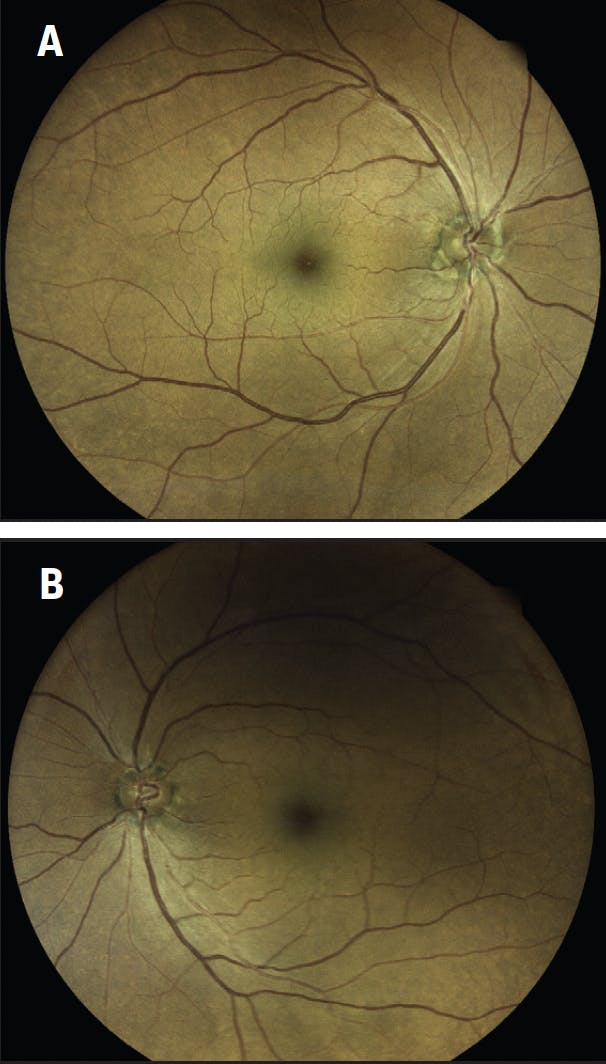
Figure 2. A fundus examination reveals a relatively healthy RNFL in the right (A) and left (B) eyes.

Figure 3. OCT scans of both eyes show a normal RNFL in the right eye but poor image capture in the left eye because of corneal pathology.

Figure 4. Visual field tests of the right (A) and left (B) eyes show inferior artifacts thought to be due to corneal pathology.
The patient desires improved vision and comfort. What do you think is the likely cause of his corneal pannus? How would you evaluate his testing and grade his glaucoma? How would you manage this patient?
—Case prepared by Jacob Brubaker, MD
DEBORAH RISTVEDT, DO
Corneal scarring and pannus without a history of contact lens wear, chemical injury, infection, or trachoma makes me think of chronic inflammation that has led to keratitis and subsequent scarring over time. I would check this patient’s corneal sensitivity for a possible neurotrophic component.
In this case, keratoconjunctivitis sicca from topical medical therapy and Terrien marginal degeneration would be high on my list during the differential diagnosis. Given the stated unreliability of OCT imaging and visual field testing, serial optic nerve photography and a direct examination of the RNFL are options for monitoring this patient.
Corneal irregularity and scarring, moderate anterior chamber depth, a history of using multiple glaucoma medications, and phakic lens status are key factors to consider when deciding how to manage this patient. Because his optic nerves appear to be relatively healthy, I would initiate aggressive treatment for ocular surface disease and attempt to reduce the burden of medical therapy and address the corneal irregularity. I would perform cataract extraction to deepen the angle, followed by angle surgery to lower the IOP and decrease the number of glaucoma medications the patient requires. A scleral contact lens would be fit to address corneal irregularity and quality of vision.
Improved visual acuity and quality of vision may make visual field testing more reliable and facilitate monitoring this patient for glaucomatous progression over time.
MANJOOL SHAH, MD
The exam findings demonstrate significant ocular toxicity to topical agents manifesting as limbal stem cell loss. The treatment plan therefore requires close partnership with a cornea specialist.
All topical agents would be discontinued. Conservative management of the cornea would include the use of preservative-free artificial tears, warm compresses, and lid care. I would also consider initiating treatment with low-dose preservative-free topical steroids and/or topical cyclosporine 0.05% (Restasis, Allergan).1
Considering his grade 1 to 2 angles and PAS, the patient was likely diagnosed with primary angle closure by his other provider. Grade 1 to 2 angles, however, are technically open. Because four classes of medication are required to achieve an IOP of 19 mm Hg, I would treat this case as open-angle glaucoma. Fortunately, optic disc photography suggests minimal optic neuropathy, so the patient can likely tolerate an increase in IOP from a topical drug washout. Oral carbonic anhydrase inhibitors or selective laser trabeculoplasty could be considered as temporizing measures while the ocular surface stabilizes. Unfortunately, given the anterior chamber anatomy, an intracameral bimatoprost implant (Durysta, Allergan) is contraindicated.
Ultimately, glaucoma surgery will be required, but this patient will be best served if his corneal health is optimized first. If conservative management fails, the significant corneal pannus and neovascularization may require limbal stem cell transplantation. Once the ocular surface has stabilized, glaucoma management could take the form of phacoemulsification combined with a trabecular meshwork–based MIGS procedure. I would recommend goniosynechialysis and either the placement of trabecular microbypass stents or an excisional goniotomy. I am concerned that the PAS indicate areas where Schlemm canal has collapsed. If a trabecular meshwork scaffolding microstent is preferred, an ab interno canaloplasty procedure could be performed first to ensure canal patency.
WHAT I DID: JACOB BRUBAKER, MD
This case illustrates the severe side effects sometimes caused by topical glaucoma therapy. I was unable to obtain this patient’s medical record detailing his maximum pretreatment IOP. Regardless, his glaucoma was quite mild and likely overtreated. The pannus was due to long-term medical treatment that was continued despite a significant topical allergy.
My first step was to discontinue the fixed-combination agent and the brimonidine. On examination 3 weeks later, the conjunctival injection had decreased, and the patient’s visual acuity had improved to 20/30 OD and 20/50 OS. Because the IOP was 17 mm Hg OD and 13 mm Hg OS, I felt we could try discontinuing bimatoprost as well. Three weeks later, the IOP was 20 mm Hg OD and 19 mm Hg OS, and the patient’s visual acuity was 20/30 OD and 20/40 OS. Unfortunately, 6 months later, the IOP had increased to 25 mm Hg OD and 21 mm Hg OS.
We had established that topical therapy was to be avoided. The patient and I therefore discussed the options of selective laser trabeculoplasty or cataract surgery combined with MIGS. He elected to proceed with cataract surgery and a 100º goniotomy performed with a Kahook Dual Blade (New World Medical) in each eye.
Postoperatively, the patient did well. One year after surgery, the IOP was 15 mm Hg OD and 13 mm Hg OS, and his visual acuity was 20/20 OD and 20/25 OS on no medication. The pannus had improved in each eye compared to his initial presentation (Figure 5). Although the patient is somewhat hampered by the residual effects of the pannus, he is grateful that he sought a second opinion.

Figure 5. Corneal pannus in the right (A) and left (B) eyes 1 year after the discontinuation of topical glaucoma therapy.
1. Kim BY, Riaz KM, Bakhtiari P, et al. Medically reversible limbal stem cell disease: clinical features and management strategies. Ophthalmology. 2014;121(10):2053-2058.




