My friend Rajamani Muralidhar, MD, MRCO, FRCS, a glaucoma specialist in Coimbatore, India, told me about Pradeep, a 16-year-old patient with severe steroid-induced glaucoma. Pradeep is the same age as my son, and his story reminded me of how challenging glaucoma can be around the world. Pradeep had been living in southern India with severe steroid-induced glaucoma from a history of steroid use for vernal keratoconjunctivitis. Figure 1 shows his visual fields at presentation. For a teenager with such significant functional damage, the prognosis was guarded. It seemed that something profound would be required to improve Pradeep’s chances of having a successful life and a career.
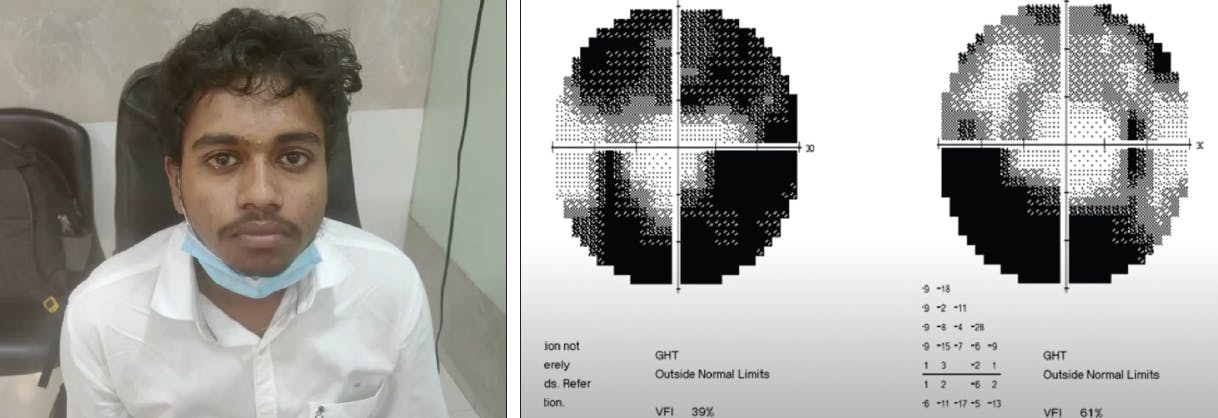
Figure 1. Pradeep had been living in southern India with severe steroid-induced glaucoma from a history of steroid use for vernal keratoconjunctivitis. For a teenager with such significant functional damage, the prognosis was guarded.
Many individuals around the world are in situations like Pradeep’s, and the global glaucoma burden continues to worsen. Glaucoma is the number-two cause of blindness and the number-one cause of irreversible blindness around the world. It is estimated that 112 million people worldwide will have glaucoma by 20401; with the 3.54% global prevalence of glaucoma1 and a projected world population of 9.8 billion,2 by 2050 the number of people worldwide with glaucoma may reach almost 350 million.
In 2021, The Lancet Global Health Commission on Global Eye Health published a report on the impact of visual impairment and blindness around the world and the importance of eye health.3 In reviewing the challenges associated with glaucoma specifically, the authors noted that, “Glaucoma lacks a one-stop solution such as cataract surgery, because of its chronic nature and complexity of management. In the absence of simple and affordable diagnostic and treatment solutions, the global eye health community has not [prioritized] glaucoma … .” In low-income and middle-income countries, more than 90% of patients with glaucoma are not receiving care.3
The task of conquering this growing issue is monumental; however, this is a crucible moment for the glaucoma subspecialty and for the world.
WHY CARE?
As has been made evident in the past 5 to 10 years, the world is increasingly connected. COVID-19 posed a universal threat to the lives and livelihoods of people all over the globe. Climate change is a threat everywhere. Civil and political unrest have consequences on an international scale. Events in all corners of the world can affect us as individuals, wherever we live.
In 2015, all United Nations (UN) Member States set forth 17 Sustainable Development Goals and outlined a plan to achieve them by 2030 (Figure 2). All these objectives are important for achieving prosperity and reducing poverty, but many of them share another common thread: 12 of the 17 UN’s Sustainable Development Goals intimately involve vision care and vision health. By addressing the global burden of glaucoma and making an impact on vision health, we have an opportunity to not only change lives but also improve development and reduce disparities around the world.

INTERVENTIONAL SUCCESSES
Several recent insights into and advances in interventional glaucoma care show promise for addressing the disease on a global scale.
As shown by the Laser in Glaucoma and Ocular Hypertension (LIGHT) trial, patients who are treated early with selective laser trabeculoplasty (SLT) are less likely to experience disease progression and have a substantially reduced risk of needing incisional glaucoma surgery.4 The 6-year LIGHT outcomes specifically showed that 69.8% of patients treated with SLT had an IOP that was at or below target, without needing medical or surgical treatment, and more eyes in the drops arm exhibited disease progression than in the SLT arm (26.8% vs 19.6%, respectively; P = .006). Further, trabeculectomy was required in 2.4% of eyes in the SLT arm and 5.8% of eyes in the drops arm. In the HORIZON study, the cumulative risk of incisional glaucoma surgery at 5 years was lower in patients who were implanted with the Hydrus Microstent (Alcon) after successful cataract surgery compared with patients who underwent cataract surgery alone (2.4% vs 6.2%, respectively; P = .027).5
It is exciting to have access to treatments that significantly reduce patients’ risk of needing incisional glaucoma surgery. However, the data suggest that many patients will continue to progress because of variability in IOP control. In the Advanced Glaucoma Intervention Study (AGIS), the odds of visual field progression went up by 30% for every 1-mm Hg increase in IOP.6 However, it is not enough to just have a set IOP; it is also essential to lower IOP. In the Collaborative Initial Glaucoma Treatment Study (CIGTS), the odds of visual field progression were 96% greater if the IOP range fluctuated above 8.5 mm Hg.7
NECESSARY TOOLS
With the aforementioned insights in mind, addressing glaucoma on a global scale will require better tools, such as continuous IOP monitoring. Although broad use of this diagnostic approach is ambitious and could be costly, it is needed to get ahead of the curve.
Three intraocular measurement tools are available from Eyemate: (1) the Eyemate-IO Implant, which is placed at the time of cataract surgery; (2) the Eyemate-SC Implant, which could be placed in the suprachoroidal space at any time; and (3) the Eyemate-IO/KP Implant for patients with a Type 1 Boston keratoprosthesis. Additionally, my colleague Bruce Gale, PhD, of the University of Utah’s School of Engineering, has developed a microfluidic chip–based IOP sensor that could be placed in the subconjunctival space. This is the type of innovation needed to identify patients with IOP variability and to ultimately reduce the burden of glaucoma around the world.
Although MIGS is efficacious, there is a ceiling to the procedures’ IOP-lowering effect. I am therefore excited about the different options emerging for blebless glaucoma surgery, including the Miniject (iStar Medical), the CycloPen (Iantrek), and the Cilio-scleral Inter-positioning Device known as the CID (Ciliatech). The CID can be used to address patients with open-angle glaucoma as well as those with closed-angle glaucoma—one of the most vulnerable groups of patients at risk of blindness. This option may prove to be a promising new approach to reduce the need for incisional glaucoma surgery.

CONCLUSION
Talking about global glaucoma can be painful, but this is our moment as a community. An intense amount of collaboration among scientists, clinicians, industry members, and patients will be required to address disparities in vision health and care and to reduce the disease burden worldwide.
Pradeep had been treating his glaucoma with four drops, but this regimen reduced his IOP to only the low 20s mm Hg. Eventually, Pradeep underwent successful gonioscopy-assisted transluminal trabeculotomy (GATT). His IOP is now in the middle-teens without medication. Pradeep has hope because of interventional glaucoma. Replicating this outcome for the many patients in need is no easy feat, but it is certainly an objective worth pursuing. Ultimately, as my mentor Alan S. Crandall, MD, once said, “It’s the right thing to do.”
1. Tham YC, Li X, Wong TY, Quigley HA, Aung T, Chen CY. Global prevalence of glaucoma and projections of glaucoma burden through 2040: a systematic review and meta-analysis. Ophthalmology. 2014;121(11):2081-2090.
2. World Population Prospects. United Nations. 2017. Accessed January 18, 2023. https://population.un.org/wpp/publications/files/wpp2017_keyfindings.pdf
3. Burton MJ, Ramke J, Marques AP, et al. The Lancet Global Heath commission on global eye health: vision beyond 2020. Lancet Glob Health. 2021;9(4):e489-e551.
4. Gazzard G, Konstantakopoulou E, Garway Heath D, et al; LiGHT Trial Study Group. Ophthalmology. 2022;S0161-6420(22)00732-1.
5. Ahmed IIK, De Francesco T, Rhee D, et al; HORIZON Investigators. Long-term outcome from the HORIZON randomized trial for a Schlemm’s canal microstent in combination cataract and glaucoma surgery. Ophthalmology. 2022;129(7):742-751.
6. The AGIS Investigators. The Advanced Glaucoma Intervention Study (AGIS): 1. Study design and methods and baseline characteristics of study patients. Control Clin Trials. 1994;15:299-325.
7. Musch DC, Lichter PR, Guire KE, Standardi CL. The Collaborative Initial Glaucoma Treatment Study: study design, methods, and baseline characteristics of enrolled patients. Ophthalmology. 1999;106(4):653-662.


