In the United States, nearly half of individuals with glaucoma say that their medications are unreasonably priced and that cost is a key reason they are unable to adhere to a glaucoma management plan.1,2 Under Medicare Part D, glaucoma medications incur the highest cost of all classes of ophthalmic medications. Glaucoma alone accounted for more than 40% of all US ophthalmic medication expenditures from 2015 to 2016.3,4
Glaucoma specialists should recognize the financial challenges that patients encounter and consider their impact on patients’ commitment to treatment. Medication adherence has been estimated to be as low as 20% in patients with glaucoma, and the consequences are clear: Decreased medication adherence is linked to a stepwise decline in mean deviation of visual fields.2,5 Furthermore, ensuring optimal medication adherence early on is essential, as adherence behavior during the first year of treatment may forecast long-term medication compliance and subsequent outcomes.6 This article explores strategies to address the financial aspects of nonadherence to glaucoma medications.
COLLABORATE WITH PHARMACISTS
Pharmacists are often very knowledgeable about patient resources for improving medication affordability. It may be worthwhile to inquire whether they know of any specific pharmacy or mail-in programs that can decrease the overall cost of patients’ glaucoma medications. Furthermore, once a new medication has proven to be effective and tolerable for a patient, prescribing them a 90-day supply may be a more economical option. Systematic reviews have found that a 90-day prescription improves medication adherence compared with a 30-day supply for many chronic conditions, including diabetes, depression, and atherosclerotic cardiovascular disease, although this trend has not been specifically evaluated for glaucoma.7
At the University of Chicago Medicine, we piloted an initiative with our institutional pharmacy during the COVID-19 pandemic to help reduce our patients’ out-of-pocket costs. In the first 2 years, we were able to process 568 formulary inquiries on behalf of 326 patients to help guide medical decision-making and provide transparency for out-of-pocket costs as their glaucoma medical management escalated.8 With this initiative, a pharmacy medication access referral order could be placed in the electronic health record to determine out-of-pocket expenses of glaucoma medications (Figure). As a result of this workflow, we identified medications that were covered by each patient’s individual insurance carrier at the lowest price possible by preemptively applying for prior authorizations, formulary exceptions, or tier exceptions. Prior authorizations often delay care and incur up to $100 in indirect costs in technician time, paperwork filing, and other responsibilities.9
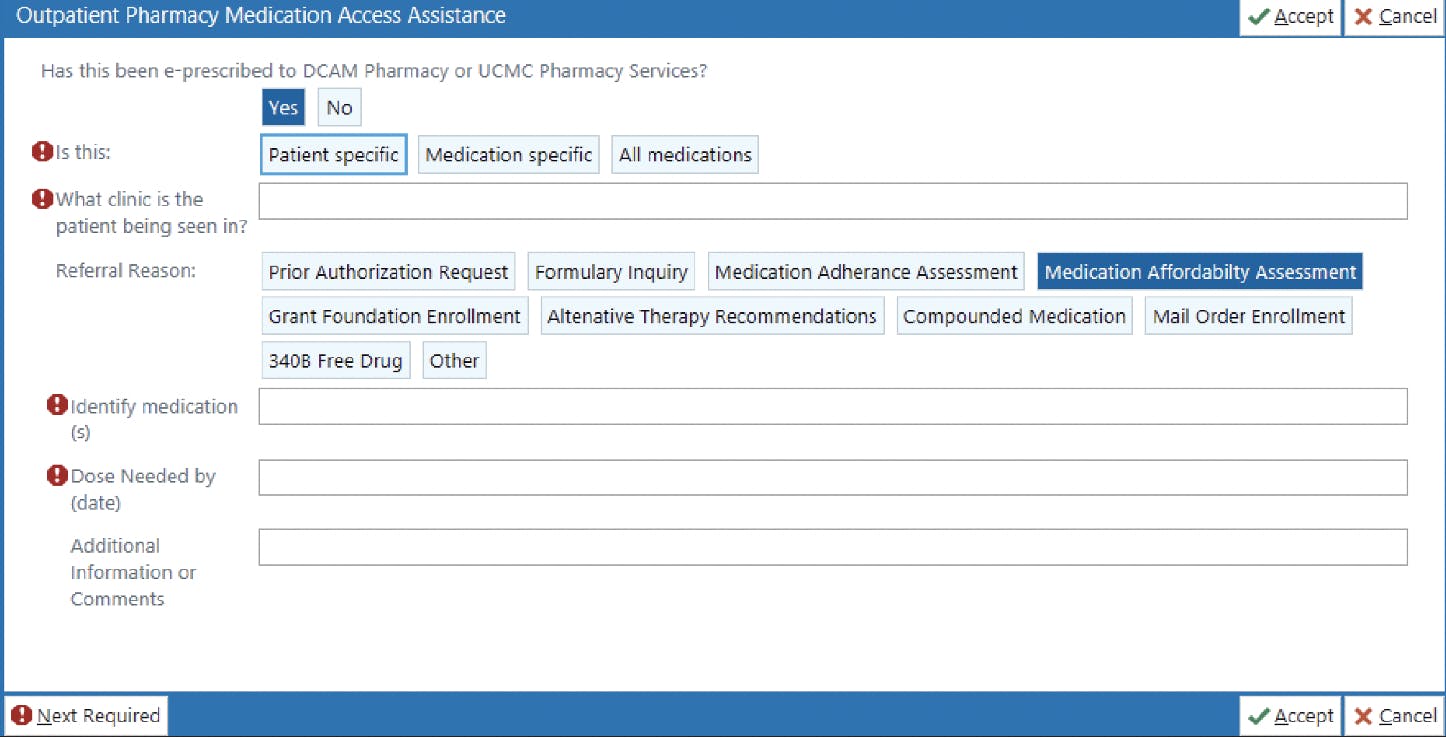
Figure. Example of the Outpatient Pharmacy Medication Access Assistance order in the electronic health record system used at the University of Chicago Medicine. Providers can communicate directly with the outpatient pharmacy to assess whether certain glaucoma medications can be attained at an affordable cost before prescribing them to the patient.
To improve efficiency, providers can designate a specific staff member to handle prior authorizations, ideally one who has language-specific skills, experience with paperwork, and knowledge of appropriate contacts. This approach ensures a streamlined process by avoiding the need for a new person to learn the intricacies of the process each time. Furthermore, implementing a dedicated phone line for pharmacies or insurance companies can simplify the process and prevent miscommunication.
Out of the 568 formulary inquiries we analyzed, 123 (22%) were identified to be at an acceptable cost for the patient and were successfully added to their medication regimen. After confirming that a particular medication was accessible and affordable for the patient, the glaucoma specialist would discuss the option and offer to prescribe it. This transparent workflow has the potential to improve medication adherence and glaucoma management by directly addressing a significant barrier to access.
As more data are gathered on patients’ experiences with this approach, we are eager to expand outreach of this program to more individuals on the South Side of Chicago, a metropolitan region with a high proportion of medically underserved neighborhoods and patients who experience significant financial hardships.
BALANCE GENERIC WITH BRAND-NAME MEDICATIONS
From 2013 to 2019, after adjusting for inflation, brand-name medication expenses increased by 59%, whereas generic drug costs declined by 22% within the same timeframe.3 Nearly 80% of glaucoma medication costs under Medicare Part D in 2017 were attributed to brand-name medications, which were 13 to 162 times more expensive than their generic equivalents. In glaucoma care, remaining cognizant of the available generic medications as they come onto the market can make a tremendous difference. On the other hand, if the medication exists only as a brand-name drug or if the patient cannot tolerate alternatives, documenting side effects and efficacy is crucial in expediting insurance coverage. Additionally, some manufacturers will offer coupons or copay assistance for eligible patients.
EXTEND LIFESPAN OF OR REDUCE NUMBER OF MEDICATIONS
In addition to reducing the price-per-medication, other strategies to improve affordability include extending the lifespan of each bottle and reducing the number of medications prescribed. Ensuring that patients correctly administer their drops is important not only at the initial visit but any time it seems the patient may be running out of medications too quickly or they mention cost as a barrier. A 30-second video showing proper drop administration or a website link shared at check-out can improve patient education and retention of proper technique. Furthermore, for the right patient, it may be reasonable to recommend an eye drop bottle adapter such as the Nanodropper (Nanodropper) to increase the number of drops per bottle. (Editor’s note: For more information on drop aids, see “Advances in Eye Drop Aids” on page 34.)
Finally, being proactive about offering selective laser trabeculoplasty (SLT) can go a long way in reducing medication burden. We use the terms laser or surgery sparingly; rather, we simply describe the procedure, such as by saying, “We use light energy to improve the drainage channels in your eyes.” Describing the successful track record and tangible benefits of SLT can further facilitate patient readiness. For example, mention that many patients can decrease their number of prescribed medications following SLT or that the procedure is typically covered by insurance. To improve access to SLT, close communication and collaboration between optometrists and ophthalmologists is essential. Maintaining open communication and documenting the patient’s viewpoint saves time and streamlines the process for appropriate patients, particularly if a standardized process is in place.

CONCLUSION
Medication affordability remains one of the greatest barriers in glaucoma care today. It is a key culprit in hindering patients’ abilities to adhere to their management plan and ultimately contributes to permanent vision loss. With these strategies to address the financial aspects of glaucoma care, we hope that the next patient we see in clinic can become a success story in staving off this irreversible and debilitating disease.
1. Gupta D, Ehrlich JR, Newman-Casey PA, Stagg B. Cost-related medication nonadherence in a nationally representative US population with self-reported glaucoma. Ophthalmol Glaucoma. 2021;4(2):126-130.
2. Gatwood J, Brooks C, Meacham R, et al. Facilitators and barriers to glaucoma medication adherence. J Glaucoma. 2022;31(1):31-36.
3. Barayev E, Geffen N, Nahum Y, Gershoni A. Changes in prices and eye-care providers prescribing patterns of glaucoma medications in the United States between 2013 and 2019. J Glaucoma. 2021;30(3):e83-e89.
4. Chen EM, Kombo N, Teng CC, Mruthyunjaya P, Nwanyanwu K, Parikh R. Ophthalmic medication expenditures and out-of-pocket spending: an analysis of United States prescriptions from 2007 through 2016. Ophthalmology. 2020;127(10):1292-1302.
5. Shu YH, Wu J, Luong T, et al. Topical medication adherence and visual field progression in open-angle glaucoma: analysis of a large US health care system. J Glaucoma. 2021;30(12):1047-1055.
6. Newman-Casey PA, Blachley T, Lee PP, Heisler M, Farris KB, Stein JD. Patterns of glaucoma medication adherence over four years of follow-up. Ophthalmology. 2015;122(10):2010-2021.
7. King S, Miani C, Exley J, Larkin J, Kirtley A, Payne RA. Impact of issuing longer- versus shorter-duration prescriptions: a systematic review. Br J Gen Pract. 2018;68(669):e286-e292.
8. Choi JG, Amin P, Tarantino A, Qiu, M. Improved glaucoma medication access through pharmacy partnership: a single institution experience. Clin Ophthalmol. 2024;18:981-987.
9.Survey: patient clinical outcomes shortchanged by prior authorization [press release]. American Medical Association. March 19, 2018. Accessed May 31, 2024. www.ama-assn.org/press-center/press-releases/survey-patient-clinical-outcomes-shortchanged-prior-authorization






