CASE PRESENTATION
A 49-year-old White woman presents to the emergency department. Her left eye exhibits acute angle closure and has an IOP of 67 mm Hg. Her right eye exhibits primary angle closure and has an IOP of 27 mm Hg. The patient was diagnosed with narrow angles in 2014 but did not proceed with a laser peripheral iridotomy (LPI) at the time.
Therapy with four classes of IOP-lowering topical drops, acetazolamide, and a topical steroid is initiated. Baseline glaucoma testing shows a healthy, tilted optic nerve and a healthy retinal nerve fiber layer in each eye (Figures 1 and 2). Visual field testing is unreliable but suggests possible glaucomatous loss in the left eye (Figure 3). The following day, the patient receives an LPI in each eye, which resolves the pupillary block. The angles also improve but remain narrow with lens rise (Figure 4).



Figure 3. The reliability of visual field testing is poor, but the results suggest possible glaucomatous loss in the left eye.

One month after the LPIs, the patient’s unmedicated IOP is 12 mm Hg OU. In the left eye, the pupil has a diameter of 3 mm, and its response to light is sluggish. Two months after the LPIs, the patient presents with an IOP of 43 mm Hg OS. The iridotomy has been blocked by iridocorneal contact with some recurrence of pupillary block but no frank iris bombe (Figure 5). Repeat testing confirms visual field loss in the left eye. Therapy with acetazolamide and four classes of topical ocular hypotensive medication is initiated but fails to reduce the IOP. An urgent lensectomy is therefore performed.
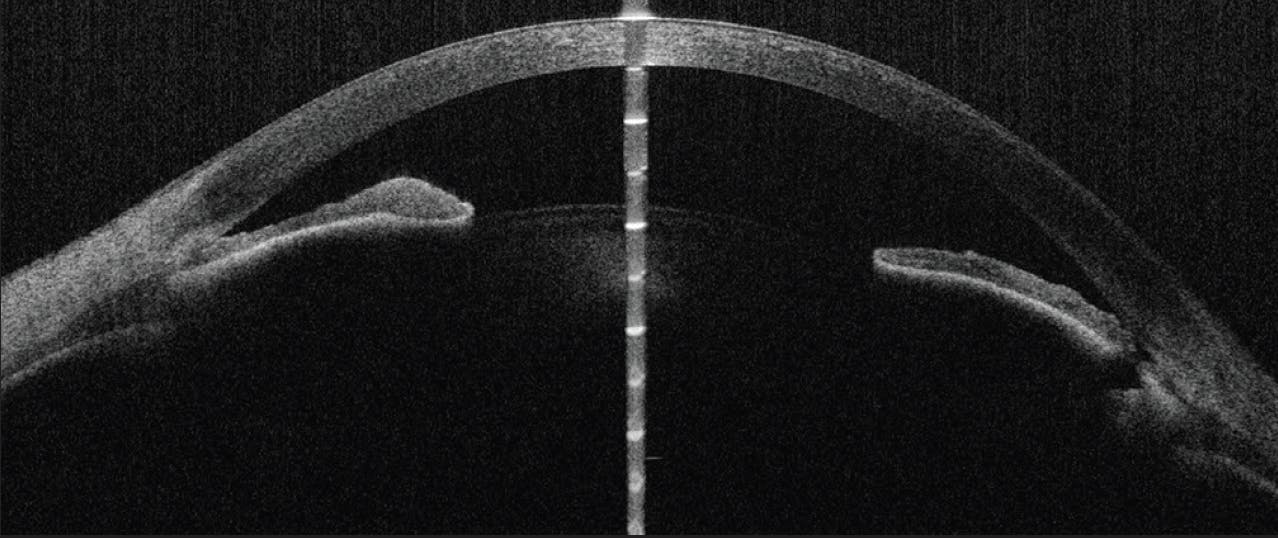
Figure 5. AS-OCT imaging of the left eye shows blockage of the LPI by iridocorneal contact and a recurrence of pupillary block.
One day after surgery, the IOP is 55 mm Hg OS. An anterior chamber paracentesis is performed, topical glaucoma therapy is continued, and pilocarpine is added to the drug regimen. One week after the lensectomy, the IOP is 40 mm Hg OS, and 360º of peripheral anterior synechiae (PAS) have developed. Structural and functional disease progression is evident (Figure 6).

How would you proceed?
—Case prepared by Devesh K. Varma, MD, FRCSC
SUNEE CHANSANGPETCH, MD, BPH
The patient has uncontrolled IOP, primary angle-closure glaucoma, progressive damage from the disease, and a history of two acute angle-closure attacks in the left eye. The underlying mechanisms—pupillary block and lens factors—were addressed by cataract surgery, but the angle has been closed by 360º of PAS.
My strategy would be to reopen the angle. The unmedicated IOP was in the low teens 2 months ago, indicating that the PAS are newly formed and IOP reduction is possible once the PAS are released. An argon laser peripheral iridoplasty (ALPI) would be performed to release the PAS. In addition, frequent administration of a topical steroid would be initiated to control inflammation from the recent surgery and acute angle closure. This therapy would also help prevent further PAS formation. A short course of acetazolamide would be restarted to lower the IOP, and the other topical medications would be continued. The patient would be asked to return for follow-up within 1 to 2 weeks to assess her response to laser treatment.
ALPI may fail to control the IOP if the iris is not released from the angle, the angle is opened to only a limited extent, or it opens but the IOP is not reduced. I would therefore counsel the patient preoperatively that further surgery may be required if laser treatment is unsuccessful.
Should additional surgery prove necessary, options include trabeculectomy and goniosynechialysis combined with goniotomy, depending on the extent of the remaining PAS, the IOP, and the condition of the conjunctiva. If the ALPI releases most of the PAS but the IOP remains high, trabeculectomy would be my next step. I would discuss the risks of the procedure with the patient. Regardless of which surgical procedure is performed second, my preference would be to defer intervention until the inflammation has lessened as much as circumstances will allow.
SHAN C. LIN, MD
Understanding the mechanisms for the angle closure might facilitate a decision on how to proceed. The anterior segment OCT (AS-OCT) images obtained before lens extraction show an exaggerated lens vault (“volcano”) configuration (Figures 4 and 5). In Figure 4, the angles appear to be closed or very narrow despite a patent iridotomy. Plateau configuration is likely also a contributing factor, especially given the patient’s age. Ultrasound biomicroscopy (UBM) could help identify additional etiologies such as plateau iris syndrome that AS-OCT imaging may not be able to detect definitively. Other anatomic causes that can be assessed by UBM include ciliary effusions, iridociliary cysts or tumors, and ciliary block.
Surgical correction is required to address the refractory IOP. In my opinion, the safest and most effective approach would be to implant an Ahmed Glaucoma Valve (New World Medical). The anterior chamber would be partially filled with an OVD, and a drop of topical atropine would be instilled at the end of the case to prevent a shallow chamber and hypotony. Depending on what UBM reveals about the mechanism(s), a goniosynechialysis could be performed before tube placement to create adequate space in the angle for device insertion.
If directed toward the posterior portion of the ciliary processes, endoscopic cyclophotocoagulation could improve the angle configuration by shrinking the processes and pulling them away from the iris (with consequent opening of the angle). The procedure could be performed concurrently with the tube shunt surgery.
Although traditional MIGS procedures such as the placement of an iStent (Glaukos) have been used successfully in cases of mixed-mechanism and narrow-angle glaucoma, I would not recommend this route given the complete closure of the angle and the severe IOP elevation.
WHAT I DID: DEVESH K. VARMA, MD, FRCSC
I suspected that the iris sphincter muscle in the patient’s left eye had been compromised by the prior acute angle-closure episode, leading to the development of PAS. I therefore performed a midperipheral iris cerclage (Figure 7) in addition to a 360º goniosynechialysis to prevent a recurrence of the PAS and mechanically open the angles further. These procedures were combined with the ab interno placement of a Xen Gel Stent (AbbVie) because I felt the trabecular meshwork might no longer be functioning adequately.

Six months postoperatively, the angles of the left eye have remained open, an unmedicated IOP of 13 mm Hg has been sustained, the bleb remains diffuse, and no disease progression has been observed.


