The theory of angle study and angle closure, including the definition of Plateau Iris, was determined with optical methods (ie, slit-lamp biomicroscopy and gonioscopy). Anything within the retroiridian space therefore was not considered because it could not be visualized due to the barrier effect of the iris. The anatomical aspects of Plateau Iris, including the retroiridian space, were examined bi-dimensionally with ultrasound biomicroscopy (UBM) for the first time in 1992, revealing the importance of the iris’ peripheral configuration.
Despite Chandler and Törnquist’s first description of this characteristic in 1958, Plateau Iris was initially observed only in patients who presented with a narrow angle, intermittent angle closure, and in some cases angle-closure glaucoma after repeated iridotomies.1-5 Today, we know that not only does Plateau Iris appear after iridotomy, but the condition has many more implications.6-8
DEFINITION AND THEORIES
According to the classic definition of Plateau Iris, the condition occurs because of presurgical changes in eyes with a normal anterior chamber depth and flat iris profile that display an extremely narrow or closed angle on gonioscopic examinations. It has also been described as an acute glaucoma crisis in one eye with a relative normal central anterior chamber depth and patent iridotomy on direct examination, presenting angle closure confirmed by gonioscopic examination after mydriasis.
Early theories explaining the Plateau Iris were only speculative. Törnquist postulated that the anomalous position or structure of the ciliary body and the contraction of the ciliary muscle could cause its anterior displacement, narrowing or closing the angle.3 Barkan postulated that the increase in the size of the lens produced peripheral closure due to a narrowing of the perilental space.1 Chandler and Grant believed that an anterior rotation of ciliary processes like what can occur in choroidal effusions or after scleral buckling surgery occurred.5 Lowe claimed that anomaly was in the size and insertion of the iris root; when the root of the iris and angle were narrow, pupillary dilation caused closure by apposition on the trabeculum of a peripherally thick iris, even with an iridotomy.
Gonioscopy provides a view of Plateau Iris, but it is performed mostly by specialists. Additionally, the iris becomes a barrier that limits the observation of all the parameters that characterize it. An anatomical configuration of the iris (ie, its insertion in the ciliary body) in closed, open, and occluded states is shown in Figure 1. These images were captured with the ABSolu UBM device (Quantel Medical by Lumibird Medical).
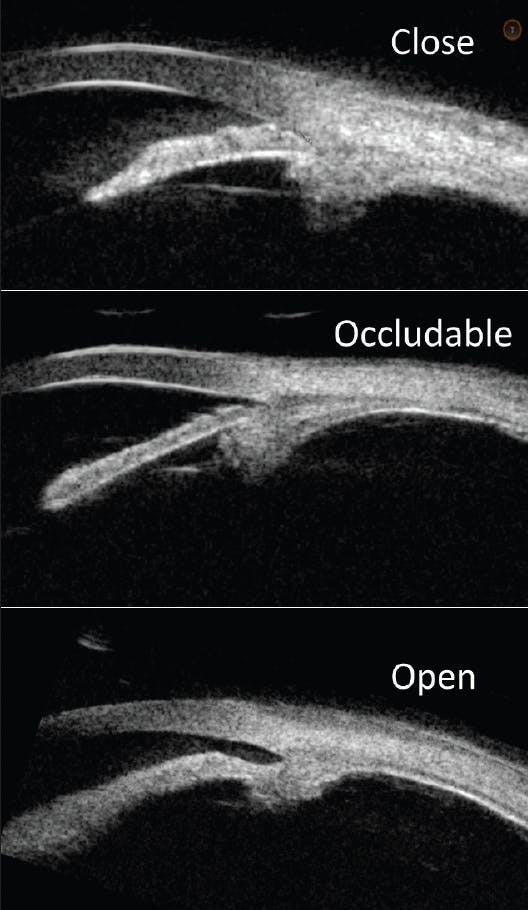
Figure 1. Images of the three types of insertion of the iris in the ciliary body that cause different angles in amplitude: Closed, occludable, and open.
Today, we know that the Plateau Iris is an anatomical configuration of the angle. It occurs more frequently than the literature indicates, especially in Southeast Asia and Latin America because it is phenotypically predetermined. Inheritance is typically an autosomal-dominant pattern with incomplete penetrance. It can be observed from an early age, but it consolidates when the anterior chamber is finished developing.9-11
The most important factor of the Plateau Iris is the insertion of the iris in the ciliary body because it determines the opening or closing of the angle and the position of the ciliary body. It is therefore the entire anterior chamber and not the position of the ciliary body that contributes to plateau iris. Even when there is pressure in the retroiridian space, as in pupillary block, the ciliary body does not advance.12,13
UBM AND IRIS PLATEAU
Unlike gonioscopy, UBM can image the dimensions and anatomical relationships of the iridocorneal angle, iris, ciliary body, and retroiridian space of the anterior chamber. The complete configuration of the iris plateau includes five features:
- No. 1. Normal or mild narrow central anterior chamber depth;
- No. 2. Flat Iris profile;
- No. 3. Iris root angulated forward peripherally;
- No. 4. Anterior ciliary body, with one-third of its volume located in front of the perpendicular line from the surface, passing through the scleral spur; and
- No. 5. Collapse of the ciliary sulcus.
Strictly defined, a Plateau Iris configuration meets all five criteria in all four quadrants. In reality, however, all quadrants are not equal.14 The structure is called Plateau Iris-like if five criteria are met in some but not all four quadrants. There are other configurations that simulate Plateau Iris by changing the configuration of the iris root. Examples include cysts of the ciliary body or iris, tumors, and angular closure by Elschnig pearls.15
Plateau Iris configuration can present alone or be concomitant with a pupillary block or phacomorphic mechanism. Additionally, Plateau Iris is not always unfavorable. In certain cases when it concurs with the phacomorphic mechanism or pupillary block, the insertion of the iris root away from the trabeculum saves the patient from angle closure (Figure 2).
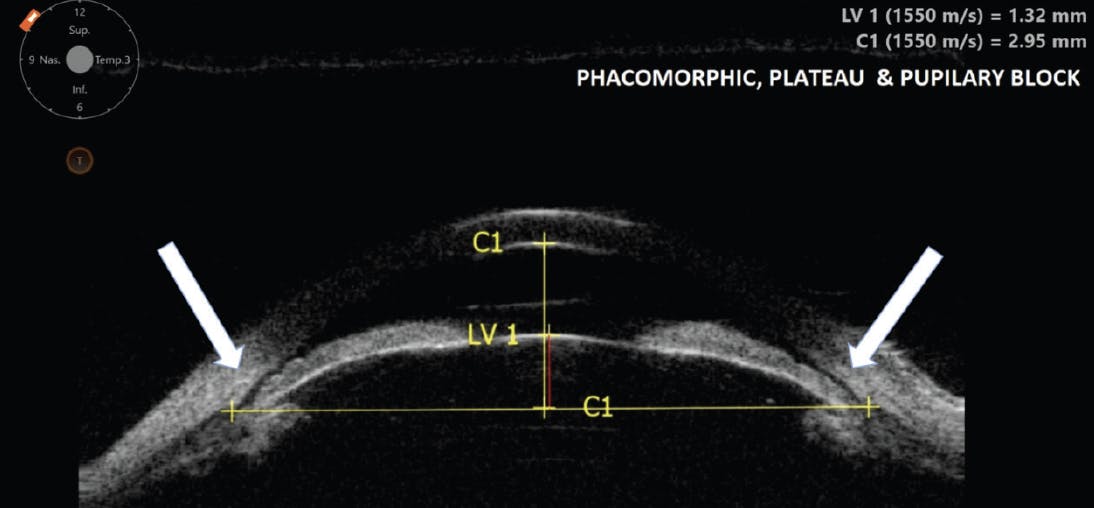
Figure 2. Combination of three risk factors for angle closure: Phacomorphic, Plateau Iris, and pupillary block. In this case, the anterior insertion of the iris into the ciliary body prevents effective angle closure.
Any narrow angle is at risk for Plateau Iris. If the condition is associated with pupillary block, an eventual iridotomy is justified. If it presents alone, however, an iridotomy is ineffective; the treatment of choice in this situation is argon laser iridoplasty, and sometimes even lens extraction (Figure 3).16
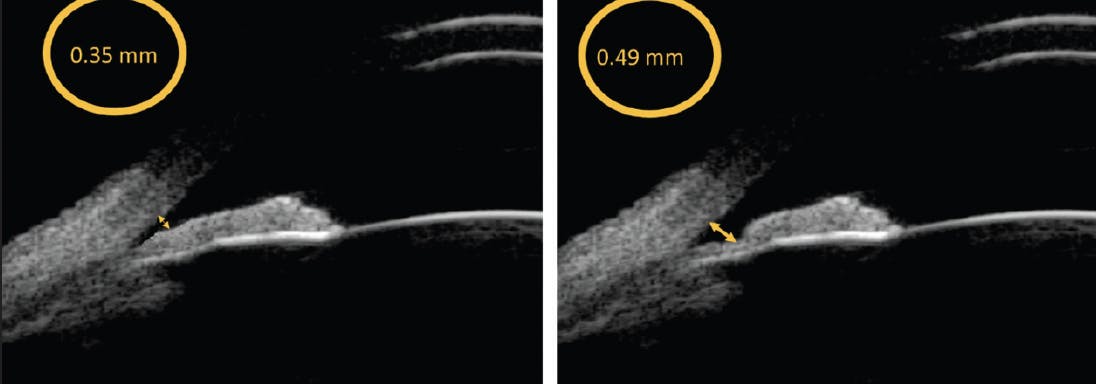
Figure 3. Iridoplasty widens the angle in the periphery, allowing a greater filtration area of the trabeculum, even a small difference in distance between the trabeculum, and the iris is hydrodynamically important for this purpose; this is seen on UBM with the ABSolu device.
CONCLUSION
UBM helps us to study Plateau Iris configuration accurately and effectively whereas optical media such as OCT of the anterior segment does not produce quality definition of the structures behind the iris, especially the ciliary body.
1. Barkan O. Narrow-angle glaucoma. Pupillary block and the narrow-angle mechanism. Am J Ophthalmol. 1954;37(3):332-350.
2. Wand M, Grant WM, Simmons RJ, Hutchinson BT. Plateau iris syndrome. Trans Sect Ophthalmol Am Acad Ophthalmol Otolaryngol. 1977;83(1):122-130.
3. Törnquist R. Angle-closure glaucoma in an eye with a plateau type of iris. Acta Ophthalmol (Copenh). 1958;36(3):419-423.
4. Kitazawa K, Nakamura Y, Nakamura C. Case of plateau iris. Ganka. 1970;12(11):939-943. [In Japanese.]
5. Chandler PA, Grant WM. Lectures on Glaucoma. Philadelphia: Lea and Febiger, 1965.
6. Ritch R. Plateau iris is caused by abnormally positioned ciliary processes. J Glaucoma. 1992;1(1):23-26.
7. Etter JR, Affel EL, Rhee DJ. High prevalence of plateau iris configuration in family members of patients with plateau iris syndrome. J Glaucoma. 2006;15(5):394-398.
8. Stieger R, Kniestedt C, Sutter F, et al. Prevalence of plateau iris syndrome in young patients with recurrent angle closure. Clin Experiment Ophthalmol. 2007;35(5):409-413.
9. Kumar RS, Baskaran M, Chew PT, Friedman DS, Handa S, Lavanya R, et al. Prevalence of plateau iris in primary angle closure suspects: an ultrasound biomicroscopy study. Ophthalmology. 2007;115(3):430-434.
10. Cronemberger S, Diniz Filho A, Ferreira DM, Calixto N. Prevalence of plateau iris configuration and morphometric findings with narrow angle or primary angle-closure glaucoma on ultrasound biomicroscopic examinations. Invest Ophthalmol Vis Sci. 2007;48:E-Abstract 3863.
11. Pavlin CJ, Harasiewicz K, Sherar MD, Foster FS. Clinical use of ultrasound biomicroscopy. Ophthalmology. 1991;98(3):287-295.
12. Pavlin CJ, Foster FS. Ultrasound biomicroscopy of the eye. New York: Springer; 1995.
13. Pavlin CJ, Ritch R, Foster FS. Ultrasound biomicroscopy in plateau iris syndrome. Am J Ophthalmol. 1992;113(4):390-395.
14. Mandell MA, Pavlin CJ, Weisbrod DJ, Simpson ER. Anterior chamber depth in plateau iris syndrome and pupillary block as measured by ultrasound biomicroscopy. Am J Ophthalmol. 2003;136(5):900-903.
15. Azuara-Blanco A, Spaeth GL, Araujo SV, Augsburger JJ, Terebuh AK. Plateau iris syndrome associated with multiple ciliary body cysts. Report of three cases. Arch Ophthalmol. 1996;114(6):666-668.
16. Ritch R, Tham CC, Lam DS. Argon laser peripheral iridoplasty (ALPI): an update. Surv Ophthalmol. 2007;52(3):279-288.
