
Sponsored by Glaukos
To watch the full webcast on Eyetube, please visit this page.
In recent years, advances in procedural interventions have enabled ophthalmologists to move the needle on proactive glaucoma management. Rather than being reactive, practitioners are aiming to intervene before patients experience major retinal ganglion cell death and irreversible visual field damage. On a recent webinar, Iqbal Ike K. Ahmed, MD, FRCSC; Arkadiy Yadgarov, MD; Sahar Bedrood, MD, PhD; and Manjool Shah, MD convened to discuss current progress and challenges with this interventional movement.
What are your thoughts on the potential limitations of topical therapy?
Dr. Yadgarov: My advocacy for interventional glaucoma care was partly inspired by a 2020 subanalysis of the Collaborative Initial Glaucoma Treatment Study (CIGTS).1 This subanalysis showed that if a patient was fully adherent to their medication regimen, their glaucoma stabilized. The disconnect is that, for decades, we've had glaucoma drops that are effective, yet patients have still been experiencing glaucomatous progression. About 50% of patients will not be as adherent or compliant as we think they are—that is a large cohort that could benefit from interventional glaucoma care. We practitioners need to do a better job with chair time and explaining why we feel that this approach works best.
Dr. Bedrood: Although it is the patient’s responsibility to take their drops as prescribed, statistics have shown that up to 90% of individuals are noncompliant (Figure 1). When I walk into an appointment, therefore, I ask myself, "What do I need to do to set this patient up for success? What do I need to do to make sure they do not lose vision?"
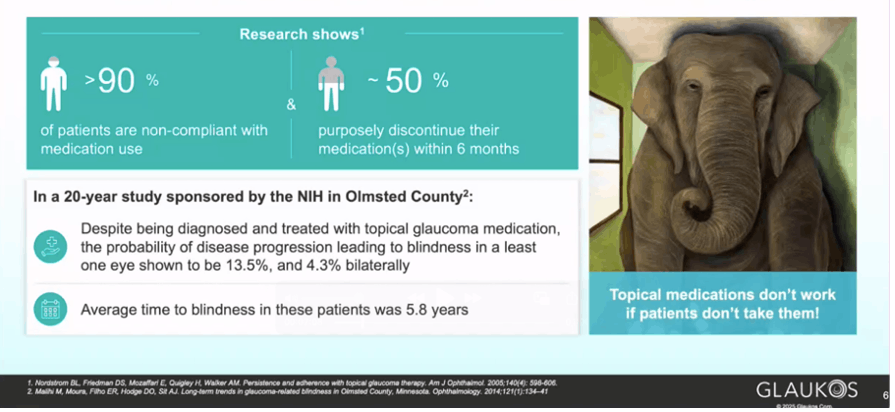
Figure 1. Rampant non-compliance and non-adherence to topical glaucoma medication contributes to disease progression
How much does quality of life play a role in interventional glaucoma? How do you communicate this to patients when thinking about the benefits of early intervention?
Dr. Bedrood: “What can I do to make this better?" is really the crux of interventional glaucoma. Whether it’s with a procedure, sustained-release drug delivery, surgery, diagnostics, etc., I believe that this should be the mindset moving forward in this space. Improving patients’ ocular surface and reducing their medication burden as much as possible are my personal goals (Figure 2). Data show that patients treated with SLT have lower IOPs over a 24-hour period than those using drops alone. That IOP control is significant.

Dr. Yadgarov: Recent innovations have been monumental in allowing ophthalmologists to approach glaucoma interventionally. Treatments such as the iDose TR (travoprost intracameral implant) 75 mcg (Glaukos), iStent infinite (Glaukos), and others are some of the most straightforward, safe maneuvers that can be used inside the eye.
Dr. Ahmed: Glaucoma is one disease for which there is no one-time, fix-all treatment. We know that interventions work better earlier in the disease course; introducing them at later stages when the disease is less treatable makes glaucoma more difficult to manage.
How do you make a case for interventional glaucoma procedures when discussing treatment options with patients?
Dr. Bedrood: The best advice I received in residency was, “Believe in the procedure you are performing.” If you believe in a procedure, practice it, understand it, and know the data, you can present it to patients and perform it with confidence, not so much as an option but rather as your professional medical opinion.
Dr. Shah: Referencing the LIGHT trial data,2 specifically visual field outcomes, we can now definitively say that there are better treatment options available than in years prior. If you believe in these improved treatments and are knowledgeable about their evidence, presenting them is not a sales pitch; it’s about doing what's right for each individual patient.
Dr. Bedrood: It is also important to talk to the practitioners who are not on board with MIGS and other procedural interventions. I would suggest they ask themselves: “What is holding me back from adopting this treatment into practice? Can I adapt it to work for my practice or maybe try a different approach?”
How do you evaluate the risk of topical drops versus the risk of early procedural intervention?
Dr. Shah: It's easy in a busy glaucoma practice to ignore the overwhelming prevalence of ocular surface disease. However, drops are certainly not benign, and it is understandable why some patients struggle with their side effects. They are a suboptimal delivery mechanism for pharmacotherapy that works, but the mechanism of administration is not ideal and not compatible with most people's lives.
Any reflections on how far we've come in glaucoma treatment and where we still need to go? How do we approach these challenges?
Dr. Shah: It is important to first recognize that we could all be managing glaucoma better. We must unburden patients of the task and rigor of managing their disease—that is our job as physicians. In terms of the specific modalities, I do not think that anyone needs to master them all. Optimize diagnostics, use early procedural intervention, and talk to patients about their medications. You will start to see that there is a place for integrating some of these procedural technologies. Nothing makes me happier than getting patients off drops and telling them, "Congratulations, we have built in the therapy into your eye." It is empowering for the patient, and that energy is infectious



