What I love most about being a glaucoma specialist today is what drew me to the subspecialty in 1986: the long-term, meaningful relationships that I have with my patients. I realize now that the very things that make a career in glaucoma challenging are what make it so rewarding.
TOUGH QUESTIONS
For every new patient I see, not only must I obtain an ophthalmologic history, but I must also pose questions regarding medical and neurologic problems that might affect visual function. I need to know about issues that could affect optic nerve function such as circulation, nutrition, and toxic exposure. I ask about things that might affect healing such as diet and medications. I inquire about medical issues that could affect long-term adherence to drug therapy such as memory loss or manual dexterity. I ferret out information about past medical problems that might have affected the optic nerve and ongoing medical problems that could determine which medical treatments are appropriate. I inquire about social issues that could affect medical therapy or even the success of a surgical procedure. It is not uncommon for a serious life event, such as the death or severe illness of a spouse, to cause a patient to forget to take medication.
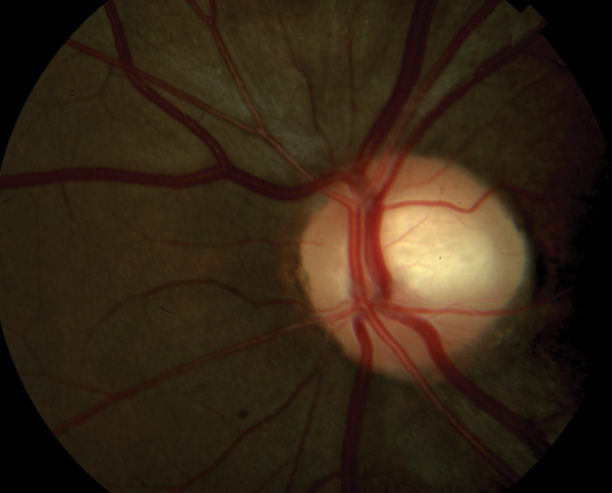
Figure 1. Optic nerve of a 24-year-old woman observed for low-tension glaucoma.
By asking often-difficult questions, I develop a clearer understanding of my patients' disease and am better able to design a therapy that will work for them. As patients open up to me about their medical and social histories, we start to form the bond that will see us both through the years of treatment ahead.
CHALLENGING EXAMINATIONS
The glaucoma examination is more challenging than a routine eye examination. The former requires a detailed evaluation of both the posterior and anterior segments, including the angle. I look for clues to secondary glaucomas that someone else may have missed or for evidence of retinal or neurologic pathology that is mimicking glaucoma. I am sure all of my colleagues have examples of patients who were monitored elsewhere for low-tension glaucoma who actually had an intracranial tumor (Figures 1 and 2).
Gonioscopy is crucial to the glaucoma evaluation yet is frequently overlooked in a general practice. The angle examination often gives me pertinent information about the cause of a patient's glaucoma and helps me to choose among possible treatment options—medical, laser, or surgical. These additional parts of the examination take extra time but frequently provide clues as to what is really happening. Many patients have thanked me for thoroughly examining their eyes. The extra time and effort build on the important relationship I have with them.
As a resident, I was fortunate to have a mentor who made clinic fun. Every day was a game of trying to find the important clue to a particular eye. Ophthalmologists must not underestimate the influence of good mentors on students or the importance of showing the enjoyment and fun of this specialty as well as its challenges.
CHALLENGING TREATMENT
Treating patients with glaucoma and cataracts requires particular skill. These eyes routinely have small pupils, weak zonules, and concurrent anterior segment disease.
Patients with uveitis often have glaucoma and pose unique challenges. Posterior segment disease can alter the red reflex and make cataract surgery more difficult.
An ability to handle these challenging cases is one of the things I love about being a glaucoma specialist. Developing these skills forced me to become a better cataract surgeon and better at communicating complexities to patients.
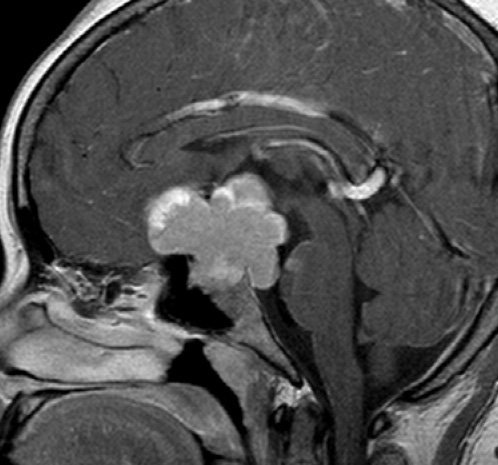
Figure 2. Magnetic resonance imaging of the same patient shows a large mass impinging on the chiasm.
PROBLEMATIC POSTOPERATIVE CARE
Glaucoma surgery is not for the faint of heart. I have always enjoyed the procedures, which require specialized skills but are fun. The real challenge is the postoperative care. Anyone who performs glaucoma surgery is well acquainted with the possible risks, complications, and frustrations. They are what make developing skillful communication skills and a trusting relationship with patients imperative.
It is important to discuss preoperatively with patients the issues that may arise so that, together, we can navigate the perioperative period with trust. This is not easy and requires time. Dealing with postoperative problems demands enormous effort, but it cements my bond with patients.
CONCLUSION
I am excited about a future in which glaucoma surgery carries fewer risks, but I believe it will still be important to build patients' trust before proceeding. I cherish the relationships developed through the years with my patients, their families, and their caregivers. They are the reason that I chose to become a glaucoma specialist, and I do not regret that decision. n

F. Jane Durcan, MD, is a partner at the Spokane Eye Clinic in Spokane, Washington. Dr. Durcan may be reached at (509) 456-0107; jdurcan@spokaneeye.com.