
Africa is disproportionately affected by blindness, with glaucoma as a leading cause of irreversible blindness throughout the continent. In one major survey, half of those known to have glaucoma had lost sight in one or both eyes.1
AT A GLANCE
• Approximately 180,000 Malawians are bilaterally blind, most often from preventable and treatable eye conditions.
• A straightforward, repeatable, and minimally invasive procedure, selective laser trabeculoplasty is particularly effective in African eyes.
• Glaucoma specialists from 16 countries work with Eyes of Africa, a state-of-the-art facility in Malawi, to educate patients, perform surgeries, and investigate glaucoma and other causes of blindness.
Malawi is one of the poorest nations in the world. Approximately 180,000 Malawians are bilaterally blind, most often from preventable and treatable eye conditions. Cataract is the leading cause, contributing to 50% of all blindness, followed by glaucoma (15%), trachoma (15%), harmful traditional eye treatment practices (6%), congenital disorders, vitamin A deficiency, and measles.1 Appropriate treatment options could prevent, diminish, or eradicate the adverse effects of these conditions. Left untreated, they create a continual source of human suffering and a substantial loss to society.
TOO FEW PROVIDERS
Watch it Now
Kaweh Mansouri, MD, of Geneva University Hospitals, Switzerland, and the University of Colorado School of Medicine, Aurora, shares principles and pearls for selective laser trabeculoplasty.

The few eye surgeons in Africa can barely address the extraordinary cataract burden that exists among urban patients with access to government-sponsored clinics. With only one ophthalmologist per million people, how can the few available regional eye surgeons care for patients with chronic ocular disorders requiring costly medication and monitoring, especially in rural areas? Even if physicians and facilities were plentiful, glaucoma would represent an enormous challenge, because African heritage is associated with a higher prevalence and greater severity of glaucoma as well as diminished drug efficacy and fibrotic healing responses compromising treatment outcomes.
Throughout the continent, low income, long distances to clinics, medical comorbidity, understaffed clinics with massive patient loads, loss to follow-up, and limited access to medications that often are not applied as prescribed may all contribute to millions of Africans’ unmitigated progression toward blindness.
PASSIVE ACCEPTANCE
The enormity of the glaucoma problem may be pushing ophthalmic practitioners into passive acceptance of vision loss from the disease. In 2010, my colleagues and I reviewed the requests submitted to Alcon Humanitarian Services, which provides supplies to medical missions around the world,3 and compared the ratio of glaucoma medications requested to the number of IOLs requested.
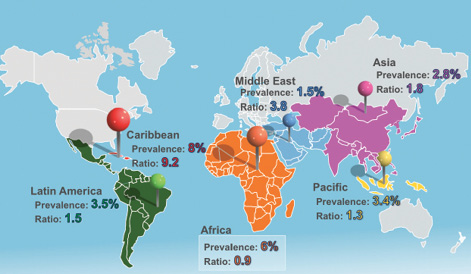
Figure 1. The ratio of glaucoma medications to IOLs that Alcon Humanitarian Services delivered in 2010.
Throughout the Caribbean (where the prevalence of glaucoma is comparable to Africa), South America, Europe, Asia, the Pacific Islands, and the Middle East, the ratio of glaucoma medications to IOLs demonstrated a strong linear association with the regional prevalence of glaucoma. Africa was the sole outlier, with a proportionate ratio of glaucoma medication to IOL requests one-tenth the level found throughout the rest of the world (Figure 1). This difference may merely reflect a mature acceptance of reality: an intermittent supply of medications is not a particularly viable solution to the African glaucoma problem.
THE HOPE OF SELECTIVE LASER TRABECULOPLASTY
Selective laser trabeculoplasty (SLT) offers the hope of positive change. A straightforward, repeatable, and minimally invasive procedure, SLT delivers a 400-µm, 3-nanosecond YAG pulse via gonio lens to the angle. In 2013, an important study showed a dramatic IOP reduction among 61 patients in St. Lucia’s ethnically African glaucoma population.2 Anthony Realini, MD, MPH, applied 100 burns and started his upward titration of power from 0.5 mJ. The outcome was truly remarkable: a sustained mean IOP reduction of approximately 8 mm Hg (> 30%) with elimination of antiglaucoma medication in 75% of subjects at 12 months.
Meanwhile, Emile Goosen, MBChB, FCOphth(SA), was supervising the use of SLT in Durban, South Africa.3 The treatment regimen used 120 to 140 burns over 360º starting at 1.1 mJ. Results among these eyes (n = 84) were similar to those observed in St. Lucia, with a mean IOP reduction greater than 30% at 12 months sustained without supplementary therapy.
The South African patient population was more diverse, however; one-quarter of the patients were ethnically Indian. The treatment responses of African and Indian eyes differed significantly. Figures 2 and 3 show the relative proportions of the African and Indian ethnic subgroups attaining an IOP reduction of at least 20%, the accepted threshold for therapeutic efficacy applied by the the American Academy of Ophthalmology and the European Glaucoma Society. Clearly, African eyes respond to SLT in a uniquely spectacular manner.
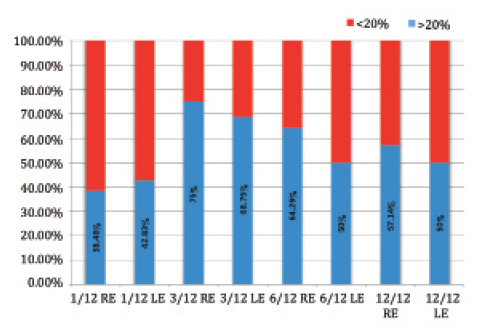
Figure 2. African patients’ IOP reduction (n = 68; right and left eyes at 1, 3, 6, and 12 months).
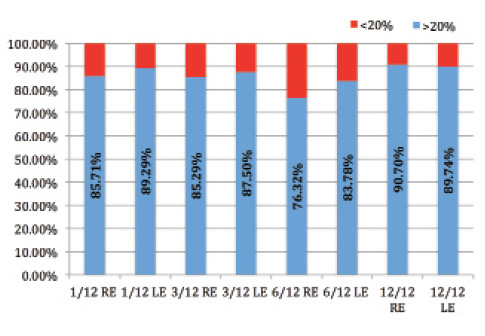
Figure 3. Indian patients’ IOP reduction (n = 21; right and left eyes at 1, 3, 6, and 12 months).
PARTNERING FOR SUCCESS
Malawi’s proactive Health Ministry actively encourages objective clinical research to optimize treatment for its populace. The University of North Carolina and Baylor University Medical Schools have been very active at the Kamuzu Central Hospital, the nation’s largest hospital complex in the capitol city, Lilongwe.
Child Legacy International (CLI), a US-based nonprofit organization, has set up operations in rural Malawi, beyond the outer limits of the nation’s electrical grid. Strategically, this would appear to be a hopeless disadvantage, but the organization’s CEO, Jeff Rogers, thankfully disagrees. Even in Lilongwe, very frequent power outages and water shortages limit the potential for any modernization of the ophthalmic care delivery system, but the Child Legacy campus, recipient of continuous solar and wind power thanks to Mr. Rogers’ efforts and ingenuity, has not had a significant power outage in more than 4 years.
The CLI staff provides a protein-deprived rural population with plentiful supplies of tilapia from their multiple excavated artificial lakes. These well-stocked lakes not only produce bulging nets of fresh fish, but they also provide irrigation for numerous hectares of newly planted fruits and vegetables that show what is possible in a nation where less than 2% of the available arable land is currently under irrigation. CLI’s hydrologic expertise does not stop at the boundaries of its educational and agricultural campus. Millions of Malawians with no prior access to clean water have benefited from CLI’s campaign to purify the water emerging from village boreholes, decimating endemic parasitic diseases.
On a relatively modest annual budget, CLI has, in less than 8 years, managed to build model facilities that now provide previously inaccessible medical care to 50,000 women and children annually. CLI’s unfettered application of modern technology in the African heartland has created an unforeseen potential to jump-start rural Malawian eye care.
Mr. Rogers’ compassionate vision and his staff’s energetic facilitation of his seemingly impossible dream are infectious, leading André Mermoud, MD, founding president of the International Society for Glaucoma Surgery, and Kate Coleman, BsC, PhD, FRCS, FRCOphth, founder of Right to Sight, to join the mission. The International Society for Glaucoma Surgery’s exective commitee, led by current president Tarek Shaarawy, MD, MSc, director, glaucoma sector, Geneva University Hospital, Switzerland, continues to enthusiastically support this project.

Figure 4. The Eyes of Africa team provides sight-saving care to thousands of rural Malawians.
In 2012, CLI partnered with the Sponsel Foundation to add a state-of-the-art eye clinic, The Eyes of Africa (Figure 4). Among those immediately involved in the establishment of this new facility was Duke University Professor Rand Allingham, MD, the primary investigator in major, National Institutes of Health-funded studies that are attempting to elucidate the biochemical character of various genes that potentiate or mitigate risk for primary open-angle glaucoma.
WELL-STOCKED CENTER
We have amassed a wide array of new, high-quality clinical and surgical equipment, now safely housed in a climate-controlled modern space. Currently set up and ready for use by regional Malawian and visiting ophthalmic teams are three phacoemulsifiers, posterior vitrectors, an optical coherence tomograph, a YAG laser, a retinal 810-nm diode laser, two xyz-zoom operating microscopes (Carl Zeiss Meditec), an A-scan with IOL calculator, and equipment for frequency-doubling technology perimetry, SLT, and photocoagulation via direct ophthalmoscopic and slit-lamp delivery systems. Major contributors to the Eyes of Africa clinic and ophthalmic ORs include the International Society for Glaucoma Surgery, CLI, Alcon, Ellex, Optovue, Iridex, IFA Systems, eye surgeons Joseph Kavanagh and Sharron Acosta, Right to Sight, VectorVision, and the Sponsel Foundation.
Recently, the Malawi Ministry of Health approved the addition of housing facilities, latrines, and a canteen for patients and families. New World Medical immediately provided a very generous donation for the construction.
HOW TO GET INVOLVED
Glaucoma specialists from 16 countries have already committed to helping educate patients, perform surgeries, and investigate glaucoma and other causes of blindness among Africans at the Eyes of Africa facilities. At press time, 36 physicians have signed up to do medical missions that last an average of 8 to 10 days. If you would be interested in forming a team or contributing your skills to help provide cataract, glaucoma, pediatric, oculoplastic, refractive, retinal, corneal, or other clinical services or to perform vital research, please contact us at Jo@saeyehealth.com. Tax-deductible donations are also welcome. Visit sponselfoundation.org to learn more.
There is much we can accomplish together, and our combined efforts with surgeons, scientists, and other professionals throughout the region can help transform eye care throughout Sub-Saharan Africa. n
1. Malawi Ministry of Health Monograph: Malawi Vision 2020 Eye Care Plan 2011-2016.
2. Realini T. Selective laser trabeculoplasty for the management of open-angle glaucoma in St. Lucia. JAMA Ophthalmol. 2013;29(3):290-297.
3. Coleman K, Visser L, Goosen E, et al. SLT as an essential tool for management of glaucoma in the African eye. Invest Ophthalmol Vis Sci. 2015;56(7):933.
William Eric Sponsel, MD
• ophthalmologist, private practice, San Antonio
• professor of biomedical engineering at the University of Texas, San Antonio
• professor of vision sciences, University of the Incarnate Word, San Antonio
• founder, Sponsel Foundation
• (210) 223-9292; sponsel@earthlink.net
• financial interest: none acknowledged