“Glaucoma patients having cataract surgery want the same thing as other patients—the best possible uncorrected vision. They want refractive cataract surgery. Toric IOLs have been amazing in helping us reach this goal. But toric IOLs are only useful in glaucoma when surgeons have the skill—and the courage—to use them.”
—Reay Brown, MD1
When considering the subject of premium IOLs and glaucoma, I am reminded of the above quote from Reay Brown, MD. Although specific to toric IOLs, these sentiments can be applied to all cataract surgery cases, especially those involving the use of premium IOLs. This article presents insights into my decision-making processes regarding refractive cataract surgery in patients with glaucoma and presents pearls for setting appropriate patient expectations and delivering on the desired results.
PREOPERATIVE WORKUP
As with standard cataract patients, I perform a comprehensive preoperative workup of all cataract patients with glaucoma. This entails a range of diagnostic evaluations, including topography, assessment of corneal higher-order aberrations, evaluation of the retina, and biometry. I then determine the status of the patient’s glaucoma using visual field testing and OCT imaging and determine which IOL options might be suitable based on their disease severity.
EXPECTATIONS MANAGEMENT
After evaluating all testing, I talk to the patient about how they want to use their eyes after surgery and how we can best meet their expectations. Glaucomatous eyes heal more slowly than nonglaucomatous eyes, so it is important to explain to the patient that their situation is unique and cannot necessarily be compared with that of their family members or friends who underwent cataract surgery. Depending on the IOL options available to the patient, they may need to be more dependent on spectacles for near or intermediate vision. If the patient is also undergoing a MIGS procedure, I advise them that their healing may take longer due to bleeding that can occur after MIGS.
A WEALTH OF OPTIONS
Surgeons today have access to a wealth of IOL options, including monofocal, monofocal toric, extended depth of focus (EDOF), EDOF multifocal, and standard multifocal with trifocal options; furthermore, mostly all of these lenses are available in toric models. This vast portfolio of IOLs enables the surgeon to fit the lens technology to the patient and not the patient to the lens technology.
Similar to this IOL portfolio, surgeons now have access to a full arsenal of MIGS procedures that can be tailored to the individual and/or combined to address glaucoma in refractive cataract surgery patients. A major advantage of MIGS is that the procedures are astigmatically neutral, so they do not affect the refractive outcomes of the cataract procedure.
DISEASE SEVERITY AND TREATMENT OPTIONS
The following scenarios illustrate the process of identifying the appropriate treatment for each patient based on their ocular health and visual needs.
Mild glaucoma. Consider a patient with mild glaucoma, who has no visual field loss, has minimal OCT progression, and whose IOP is well controlled with one medication (Figure 1). This is an individual who could be a candidate for all of the IOL options and MIGS options available today. In this scenario, the treatment decision-making should center on which approach works best in the surgeon’s hands and on the individual patient’s desires for their postoperative vision.

Figure 1. A patient with mild glaucoma and minimal visual field loss and OCT progression is likely eligible to choose from the full arsenal of IOL options and MIGS options.
Moderate glaucoma. Consider a patient with moderate glaucoma, who has some visual field loss and OCT progression and takes more than one IOP-lowering medication (Figure 2). This individual can still choose from a wide range of IOLs, but they are likely not a candidate for a multifocal lens. They could, however, do well with an EDOF IOL, toric IOL, or the Light Adjustable Lens (RxSight) with proper consent and an upfront discussion that they may not experience the same postoperative vision as someone without visual field loss. Additionally, this type of patient is a candidate for any MIGS procedure or a combination of MIGS procedures if warranted. If the patient is on multiple medications, they may need to continue to use them after surgery, depending on the severity of their glaucoma.

Figure 2. A patient with moderate glaucoma and some visual field loss and OCT progression is likely a candidate for EDOF IOLs, toric IOLs, and the Light Adjustable Lens. Any MIGS procedure or a combination of MIGS procedures can be performed, but IOP-lowering medication may be required postoperatively.
Severe glaucoma. In cases of advanced glaucoma, in which patients have severe visual field loss and OCT progression and are taking multiple medications (Figure 3), the IOL options are more limited. It is best to avoid the use of multifocal and EDOF IOLs in these eyes. However, for patients with severe glaucoma and astigmatism, it is worth discussing the option of correcting the astigmatism with a toric IOL or the Light Adjustable Lens in an effort to deliver the best distance UCVA possible. Patients with advanced glaucoma are eligible for MIGS and may benefit from a combination of MIGS procedures to yield the greatest IOP-lowering effect. Postoperative medications will likely still be required in these cases.
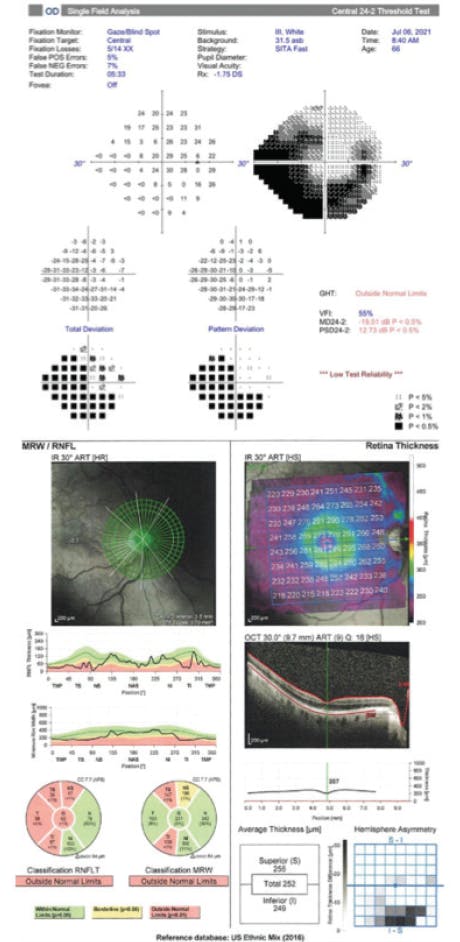
Figure 3. In a patient with severe glaucoma, visual field loss, and OCT progression, the use of multifocal and EDOF IOLs should be avoided. Options include toric IOLs and the Light Adjustable Lens. Any MIGS procedure (or likely a combined approach) can be performed. IOP-lowering medication will likely be required postoperatively.
THE REFRACTIVE END ZONE
With refractive cataract surgery, it is important to get patients into the refractive end zone. This entails delivering their desired outcome, which is typically as much independence from glasses as possible depending on the IOL they chose. Therefore, any residual refractive error or posterior capsular opacification should be addressed with a laser enhancement. After all, patients with glaucoma do not deserve the same attention to refractive outcomes as patients without glaucoma—they probably deserve more. We surgeons need to be confident, manage expectations appropriately, and deliver the desired results.
POSTOPERATIVE CARE
The postoperative care of patients with glaucoma after refractive cataract surgery is similar to after standard cataract surgery. With refractive cataract surgery, however, I pay close attention to any residual refractive errors that may be present. It is important to know the patient’s UCVA and BCVA, evaluate their IOP status, examine the anterior segment, and determine the need for IOP-lowering medication.
Day of surgery. I remind patients that their vision is likely to fluctuate on the day of surgery, especially in the evening. Additionally, there is a higher likelihood of decreased visual acuity due to blood reflux from MIGS. IOP will also fluctuate, and the patient is likely to have some corneal edema, cell and flare, and red blood cells present immediately after surgery. Personally, I stop all medications on the day of surgery because I like to reevaluate the status of the eye next day and make decisions from there. Temporarily halting medication use also simplifies the regimen for staff in the clinic and surgery center.
Postoperative day 1. On postoperative day 1, the patient’s vision will still be slightly variable, depending on their healing and on the amount of edema and blood present. In general, patients with glaucoma will have a slower healing process than standard cataract patients.
Similar to visual acuity, IOP will be variable on postoperative day 1. Patients with glaucoma are more likely to experience IOP spikes after cataract surgery. If their IOP is at target, the patient can continue without medication, although it is important to caution them that their IOP could creep up in the coming weeks.
As a rule of thumb, for patients who undergo refractive cataract surgery without MIGS, I base the postoperative care approach on certain IOP thresholds. Patients with mild or no glaucoma and IOP less than 25 mm Hg are monitored. If the IOP is between 25 and 35 mm Hg, I add medication. If the IOP is over 35 mm Hg, I may burp the wound and add medication. For patients who undergo MIGS in addition, I base my postoperative decision-making on the severity of their glaucoma. In these cases, the IOP parameters may be lower, and I may be more aggressive about adding medication to prevent IOP spikes.
On postoperative day 1, patients may have some corneal edema and red blood cells in the anterior chamber. Hyphema is possible and should be monitored, as it can decrease visual acuity and temporarily increase IOP. I inform patients of this possibility up front and communicate that any potential visual effects will be temporary. For those who develop hyphema, I warn them that they could experience sudden decreases in visual acuity but that this issue will resolve over time. It is not necessary to take the traditional traumatic hyphema cautions (eg, bedrest or additional medication) as these hyphemas will resolve over time without additional intervention.
Postoperative week 1. By 1 week postoperatively, the patient’s visual acuity should be improved and starting to stabilize. IOP should also be stabilizing. If the pressure is acceptable, the patient can be kept off medications. It is important to ensure that any hyphema is resolving.
Postoperative month 1. By 1 month postoperatively, patients who underwent standard cataract surgery should be ready to receive their new glasses prescription. If they have undergone refractive cataract surgery, this is the time to evaluate the need for any fine-tuning. A laser enhancement can be scheduled for a few months down the line to enable adequate time for healing to occur. IOP that remains elevated could indicate a steroid response. Continue to watch the patient’s medications based on their glaucoma severity and adjust the regimen as necessary. I like to set up a 3-month visit to reestablish glaucoma care and conduct new baseline tests.
Following MIGS. As I monitor these patients over time, I continue to assess the IOP, optic nerve, OCT images, and visual field tests. I continue to evaluate their medical therapy and make adjustments depending on glaucomatous progression. A few months after surgery, the refractive outcome should be stable. If any posterior capsular opacification is present and affecting the patient’s vision, an Nd:YAG laser capsulotomy around 3 months postoperatively can help them get into the refractive end zone.

Advanced Lens Technology and Glaucoma
Manjool Shah, MD, presents pearls for the use of advanced lens technology in glaucomatous
CONCLUSION
Patients with glaucoma deserve the option of refractive cataract surgery; however, IOL selection in these cases will be affected by disease severity. Modern IOLs work very well, but glaucomatous eyes have pathology that may affect the success of advanced lens technologies, so careful selection is necessary.
Overall, surgeons must have the courage to evaluate all of the treatment options available, set appropriate patient expectations, and deliver the desired refractive outcomes. Doing so can help patients with glaucoma to achieve greater independence from spectacles and potentially greater independence from their medications with the combination of refractive cataract surgery and MIGS.
1. Brown R. EyeWorld. August 2017. Accessed August 1, 2021. https://digital.eyeworld.org/i/853444/64


