Children may be the most vulnerable group that glaucoma specialists treat. Most cases of pediatric glaucoma are managed surgically, typically first with angle-based procedures. Glaucoma surgery on a pediatric patient, however, is not the same as glaucoma surgery on an adult. The small size and anatomy of children’s eyes warrant special consideration. More time and patience are needed for evaluation, decision-making, and family education on the disease, treatment options, and lifelong follow-up required.
This article shares pearls for successful pediatric angle surgery, including some useful tips for the pre- and postoperative periods.
PREOPERATIVE PEARLS
A thorough discussion with the patient’s family is the most important preoperative step. Parents should understand that more than one surgery may be required and that there is a risk of amblyopia.
Selection of the surgical method starts in the office. It may be necessary to perform an examination under anesthesia to determine the best approach. The type of glaucoma and the exam findings inform decision-making. For angle surgery to succeed, the main site of outflow resistance must be the trabecular meshwork.
A gross evaluation of corneal clarity is required to determine the appropriate angle-based procedure and whether to use an ab externo or ab interno approach. Ab externo trabeculotomy is preferred for eyes with severe corneal edema, whereas goniotomy is the procedure of choice for eyes with clear corneas. In patients with mild corneal edema, the choice of surgery may be based on an examination under anesthesia and the visibility of the angle structures in the OR (Figure 1).

Figure 1. Severe (A) and mild corneal edema with Haab’s striae (B). A corneal traction suture is placed, and the conjunctiva is opened in the superior quadrant (A).
The presence of other ocular or systemic problems should be questioned. For example, the presence of iridolenticular or iridocorneal adhesions together with a central corneal opacity in a patient with Peters syndrome (Figure 2) or choroidal thickness in a patient with Sturge-Weber syndrome should be evaluated.

The anesthesiologist should be aware of the systemic risks associated with comorbidities such as Sturge-Weber syndrome and Lowe syndrome. As such, the anesthesiologist, glaucoma specialist, and pediatrician should discuss the patient’s unique risks before the day of glaucoma surgery.
INTRAOPERATIVE PEARLS
Patient Positioning
The patient’s head must be tilted to achieve an adequate view of the angle. The surgeon should alert the anesthesiologist whenever the angle or position of the patient’s head is adjusted during the procedure.
Corneal Incisions
Long corneal incisions should be avoided because they can cause corneal striae to form during surgical manipulation and hinder visualization of the angle.
Schlemm Canal: Tackling Different Angle Anatomy and Cloudy Corneas
In addition to the smaller size and limited working space, pediatric eyes with angle dysgenesis have different ocular anatomy. An adequate view of the angle must be maintained intraoperatively, and the surgical goniolens should float over the cornea to avoid corneal distortion. The trabecular meshwork is generally harder to visualize in children because it is less pigmented, and iris insertion can be high depending on the severity of angle dysgenesis (Figure 3A–C). Further, it may be difficult to locate Schlemm canal in the presence of corneal edema or Haab’s striae (Figure 3A). Corneal edema and angle visualization may improve once the surgeon enters the anterior chamber and IOP decreases (Figure 4). Blood reflux into Schlemm canal should be checked and may enhance visualization of the canal (Figure 5). Once the goniotomy is complete and Schlemm canal has been located, the white posterior wall of the canal should be visible (Figure 3A–C).

Figure 3. Varying degrees of anterior chamber angle dysgenesis in congenital glaucoma. Mild angle dysgenesis is characterized by identifiable (A) and less identifiable (B) scleral spur with high iris insertion (arrows). The posterior wall of Schlemm canal is visible after the first goniotomy incision. Severe angle dysgenesis with higher iris insertion (C) obscures the scleral spur and trabecular meshwork entirely.
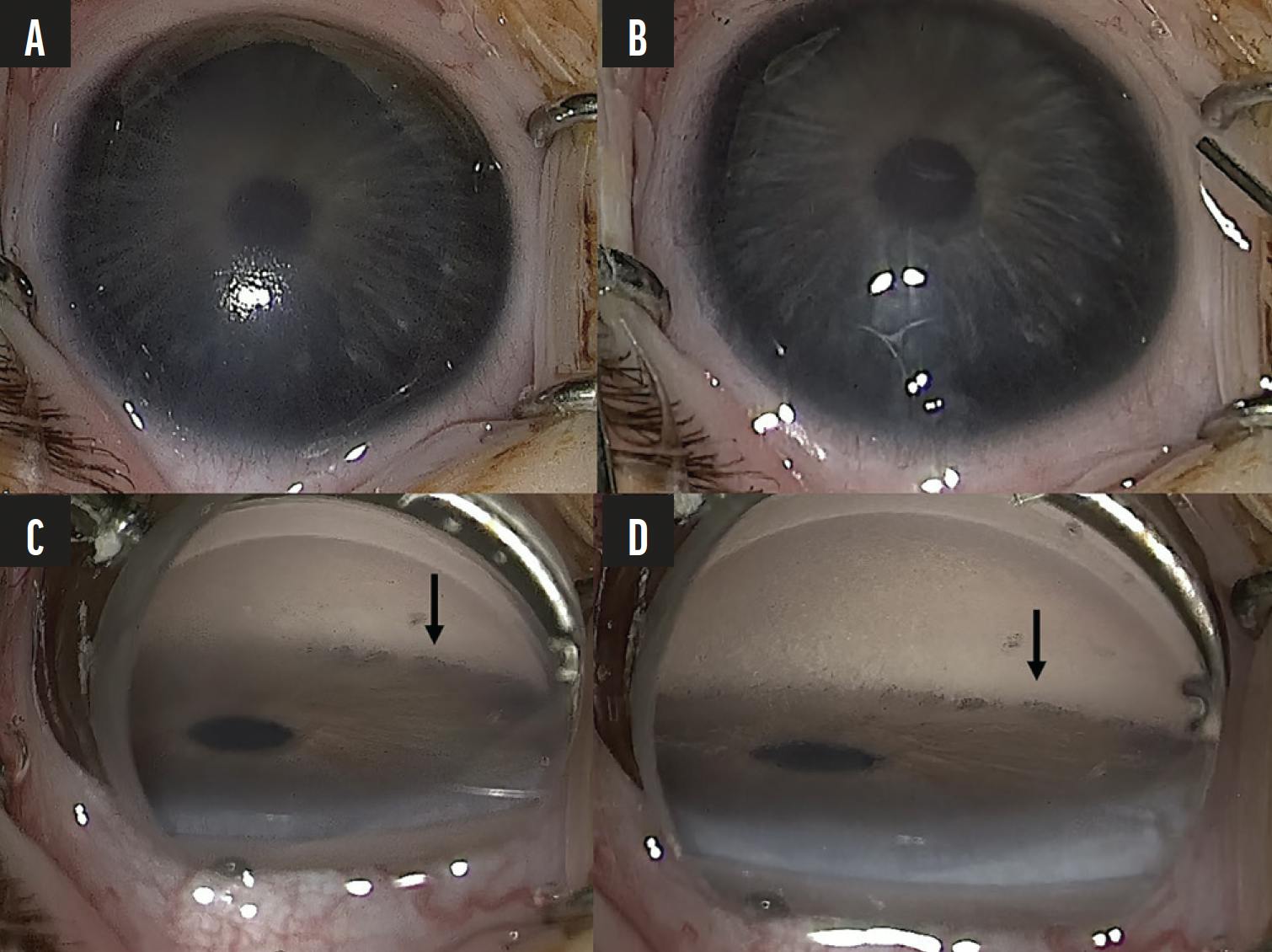
Figure 4. The paracentesis affects corneal clarity and angle visualization in a patient with primary congenital glaucoma. A preparacentesis image shows moderate corneal edema (A). The gonioscopic view prior to paracentesis creation shows hazy visualization of the angle due to stromal edema (arrow; C). A postparacentesis image shows an improvement in corneal clarity (B) with improved visualization of the angle (arrow; D).

Before starting the goniotomy in aphakic eyes, the anterior chamber is examined for vitreous by injecting triamcinolone acetonide (Figure 6). If necessary, a slight anterior vitrectomy can be performed at the start of the procedure.
To locate Schlemm canal with an ab externo approach, a small radial incision is made near the grey zone. Circumferential fibers of the scleral spur can be seen externally. Successful entry into Schlemm canal is generally associated with reflux bleeding and aqueous percolation (Figure 7A and B).
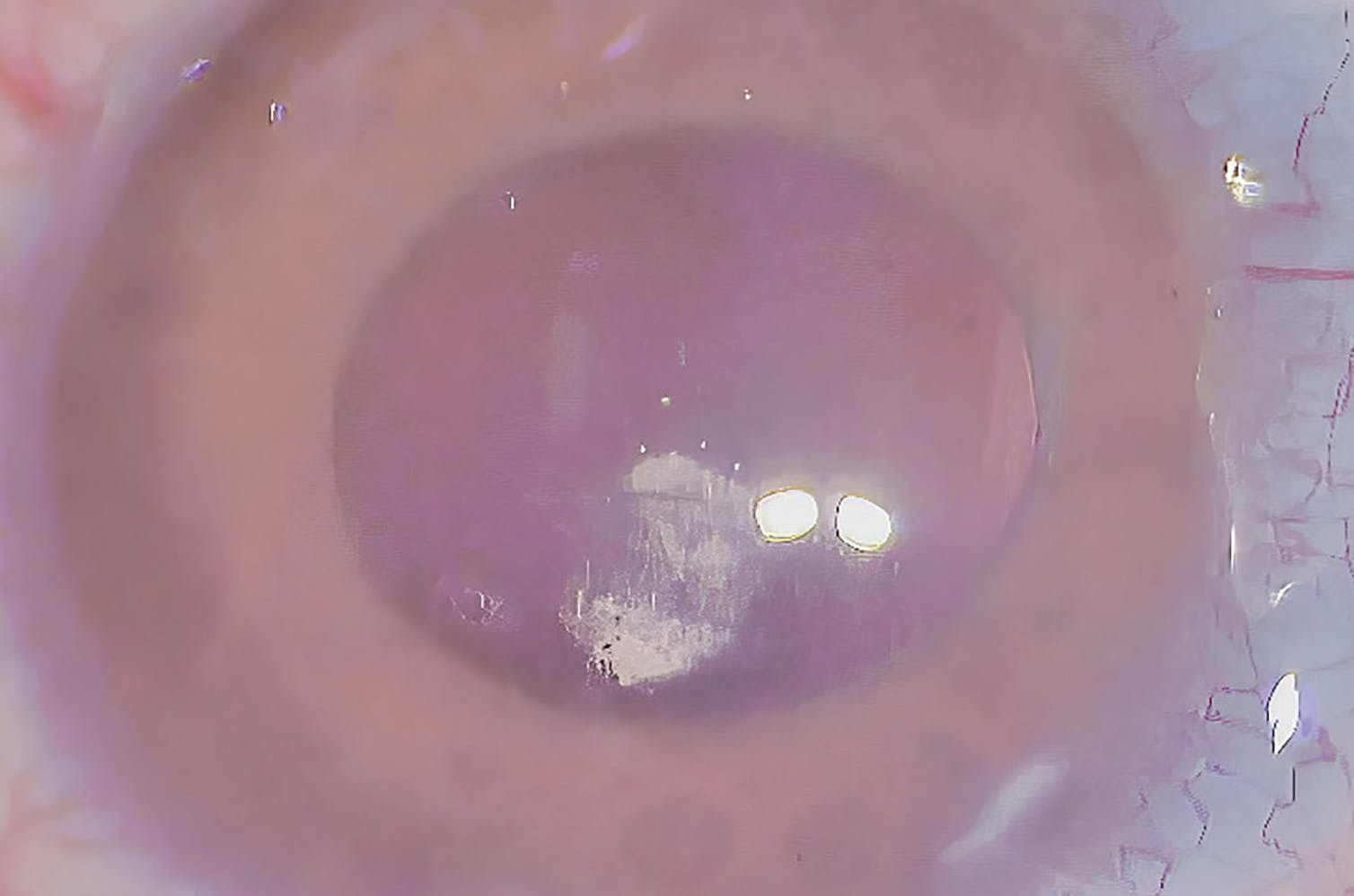
Figure 6. Presence of vitreous in the anterior chamber in a patient with aphakic glaucoma during GATT, visualized with triamcinolone acetonide.
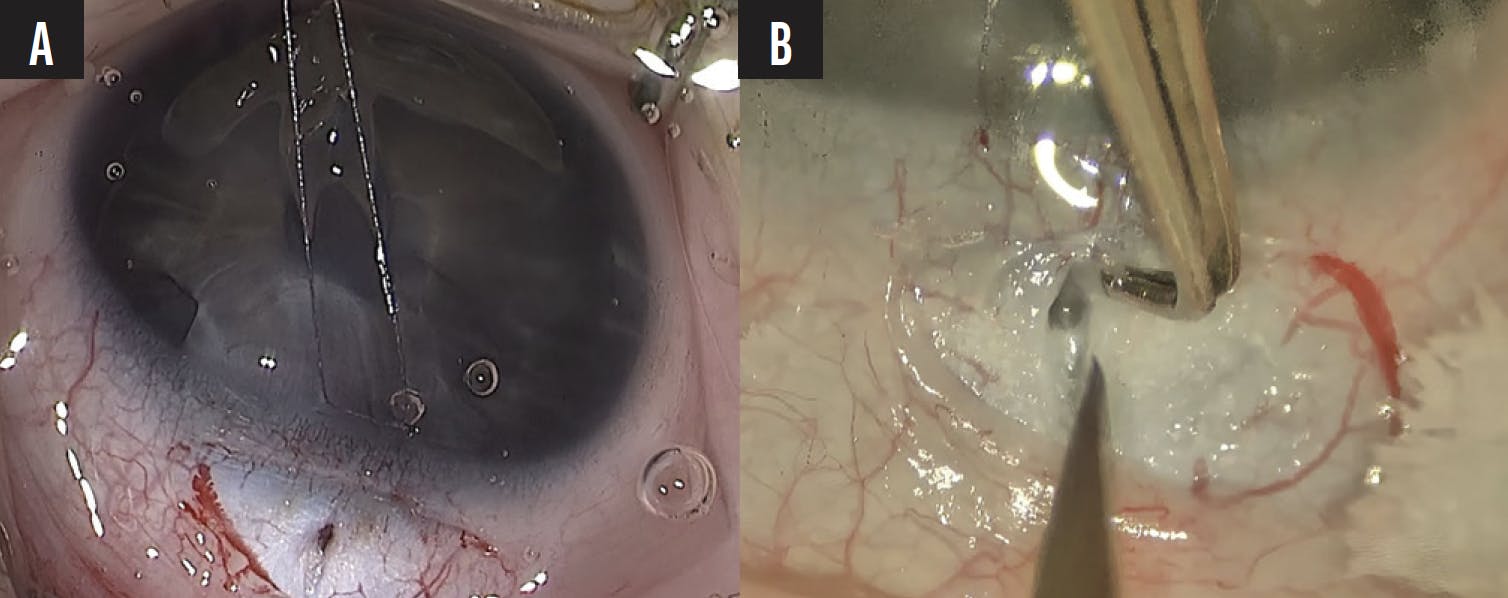
Figure 7. Intraoperative indicators of successful entry into Schlemm canal during angle-based glaucoma surgery include reflux bleeding into the canal (A) and aqueous percolation through the scleral incision site (B).
The Anterior Chamber
It is important to keep the anterior chamber wide open and pressurized throughout surgery to prevent corneal striae and reflux bleeding from Schlemm canal from obscuring the surgical view. Bleeding can also occur during the surgical manipulation of the iris in eyes with high iris insertion (Figure 8). Keeping the anterior chamber formed helps to decrease the risk of lens damage, especially in patients with aniridia.

SURGICAL TECHNIQUES
Goniotomy and Gonioscopy-Assisted Transluminal Trabeculotomy
Conventional goniotomy or gonioscopy-assisted transluminal trabeculotomy (GATT) may be performed on pediatric eyes.1-3 Once Schlemm canal has been identified, a 5-0 or 6-0 polypropylene (Prolene, Ethicon) suture with a blunt tip can be used for GATT. We prefer to use a less pliable 5-0 polypropylene suture in patients with angle dysgenesis because the material may be easier to thread, especially if Schlemm canal is not patent for 360º. A catheter with an LED light offers the advantage of visibility as it is threaded through the canal.
Once in Schlemm canal, the polypropylene suture can be seen as a blue line in the canal with the goniolens. The suture’s tip can also be observed externally in babies with thin scleras. Once the catheter has been advanced a couple of clock hours in Schlemm canal, the surgeon should stop and check the suture’s position (Figure 9A and B). It may be visible in the canal depending on the severity of the angle dysgenesis and the level of iris insertion. If the iris insertion is high, traction should be applied slowly to the polypropylene suture to avoid iris trauma and bleeding. In patients with high iris insertion, the iris should be pulled gently with forceps to allow visualization of Schlemm canal, and then a traditional goniotomy may be performed with a knife or needle.

Figure 9. A 5-0 polypropylene suture is passed through Schlemm canal in two patients with primary congenital glaucoma. The suture (arrows) is seen anterior to the iris root with blood in Schlemm canal (A) and behind the iris strands (B) in a patient with high iris insertion.
In some patients, especially those with a history of trabeculectomy or trabeculotomy, GATT can still be performed. It may not be possible to grasp the distal part of the polypropylene suture if it gets stuck in the canal at the site of the prior surgery and potential scarring. In this situation, the proximal part of the suture can be pulled, and the goniotomy may be completed in the rest of the angle (Figure 10A and B).
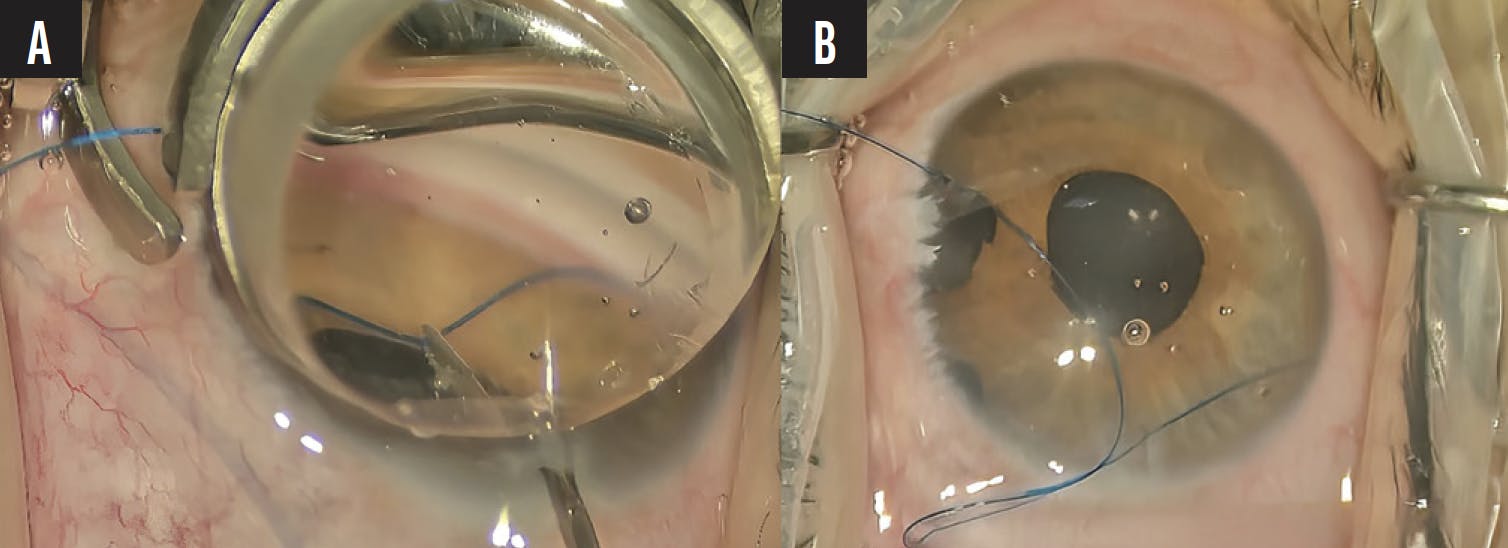
Figure 10. Intraoperative retrieval of a 5-0 polypropylene suture during GATT in a patient with primary congenital glaucoma and prior trabeculectomy. The gonioscopic view shows the distal portion of the suture stalled within Schlemm canal due to anatomic alterations from previous trabeculectomy; the proximal end of the suture is visualized and grasped near the surgical entry site (A). An external view of the same eye after successful retrieval of the suture by pulling its proximal end, with completion of trabeculotomy in the rest of the angle (B).
Trabeculotomy
Trabeculotomy is one of the most established pediatric glaucoma surgery methods. It can be performed with a Harms trabeculotome or as a circumferential trabeculotomy with a polypropylene suture. Circumferential cannulation of Schlemm canal has yielded more favorable outcomes than the traditional approach.4,5 With the conventional method, once Schlemm canal has been identified (Figure 7A and B), a Harms trabeculotome is inserted into the canal and pushed parallel to the limbus (Figure 11). The device is then rotated to avoid traumatizing the iris root and corneal endothelium.
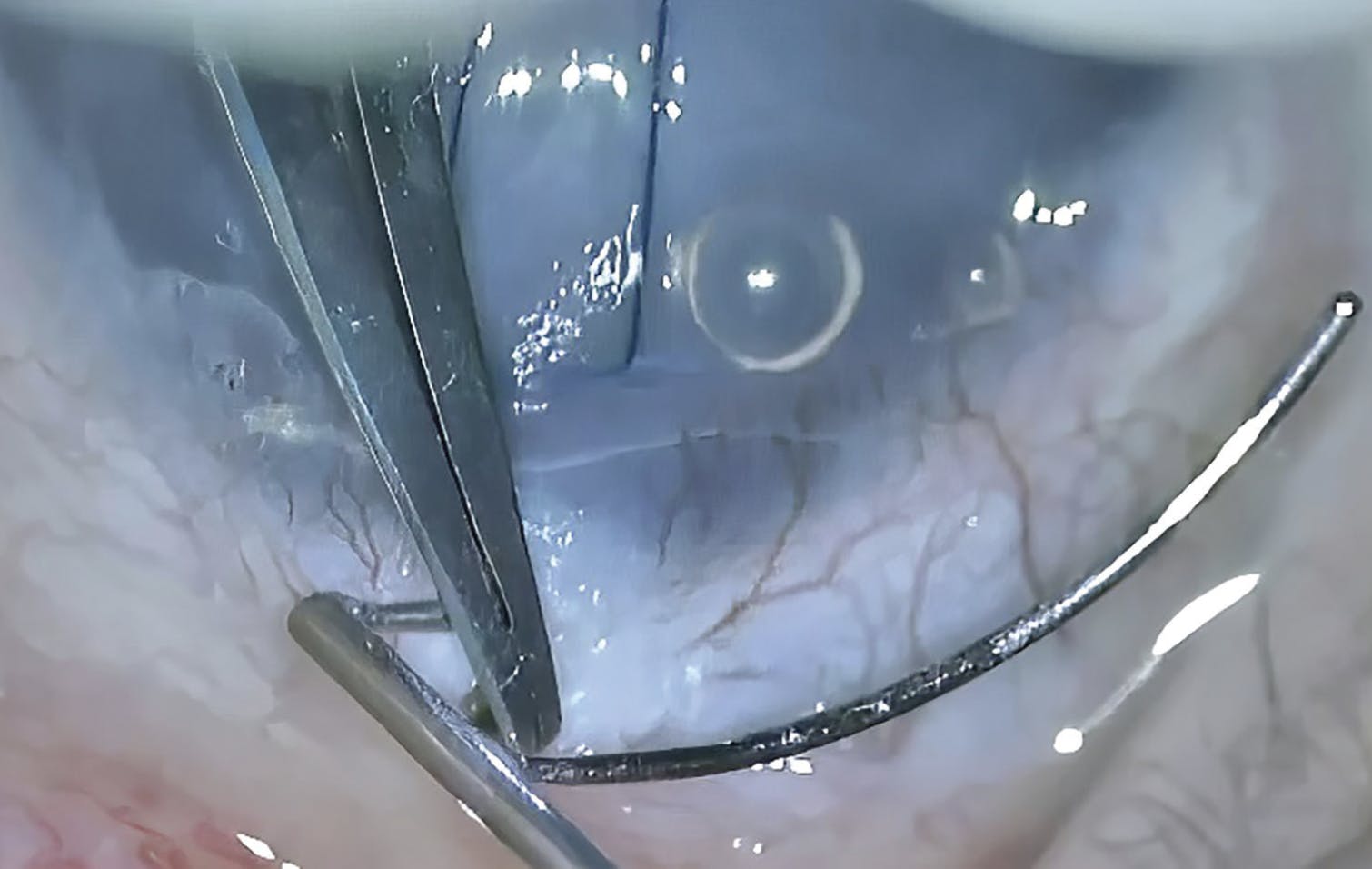
Figure 11. A conventional trabeculotomy is performed with a Harms trabeculotome, with the probe in the canal parallel to the limbus and ready to be rotated.
Combination Techniques
Different techniques can be combined to increase the extent of the angle treated. If the suture in Schlemm canal stops during GATT, the surgeon can convert to an ab externo procedure. The suture is grabbed internally at the same point if it is visible with the goniolens. Then, an ab externo trabeculotomy is performed in the other quadrants (Figure 12A and B).

Figure 12. A combined ab externo and ab interno technique for circumferential suture trabeculotomy in primary congenital glaucoma. The 5-0 polypropylene suture is introduced into Schlemm canal via an ab externo approach using a microforceps-assisted technique. Gonioscopy shows the suture (in blue) as it is advanced within and stops in the canal (A). The leading end (arrow) is retrieved ab interno using intraocular microforceps and gently pulled into the anterior chamber to complete the trabeculotomy (B).
Another approach involves combining conventional and ab externo suture trabeculotomy procedures if the suture stops in the canal. To grab and pull the proximal part of the suture during goniotomy, the suture is inserted into the anterior chamber through the trabeculo-Descemet membrane. The suture is then externalized through a paracentesis and pulled at an appropriate angle in an atraumatic way. A conventional Harms trabeculotomy can be performed in the rest of the angle to complete the circumferential goniotomy (Figure 13A–D).

Figure 13. Stepwise depiction of ab externo assisted suture trabeculotomy with ab interno retrieval and an atraumatic externalization technique. The 5-0 polypropylene suture is arrested within Schlemm canal following ab externo insertion. Advancement was halted due to anatomic resistance or canal discontinuity. The proximal end of the suture is retrieved from a separate paracentesis site using microforceps, allowing internal access to the segment located within the canal (A–B). Following successful externalization, the suture is pulled gently through the anterior chamber at an appropriate angle in a controlled manner to complete the 270° trabeculotomy (C). Trabeculotomy with a Harms trabeculotome is performed in the superotemporal quadrant to complete the circumferential trabeculotomy (D).
PEARLS FOR EARLY POSTOPERATIVE FOLLOW-UP
In the early postoperative period, topical NSAIDs or short-term steroids are administered to reduce the risk of IOP spikes, especially after GATT.6 IOP measurements are not possible in every child in the early postoperative period. IOP can be checked with digital palpation, by placing both index fingers on the closed upper lid. The amount of hyphema and the resolution of corneal edema should be monitored. Retinal complications such as choroidal effusions or vitreous hemorrhage in aphakic patients should be evaluated with ultrasound. Collaborating with other specialists facilitates effective management of complications and visual rehabilitation of the patient.
1. Aktas Z, Ozmen MC, Ozdemir Zeydanli E, et al. Efficacy and safety of gonioscopy-assisted transluminal trabeculotomy for primary congenital glaucoma. J Glaucoma. 2023;32:497-500.
2. Aktas Z, El Sayed Y, Ucgul AY, et al. Outcomes of gonioscopy-assisted transluminal trabeculotomy in children with early-onset glaucoma secondary to Sturge-Weber syndrome. Ophthalmol Glaucoma. 2025;8(4):407-413.
3. Haidu SD, Aktas Z. Gonioscopy-assisted transluminal trabeculotomy for congenital glaucoma secondary to Klippel-Trenaunay-Weber syndrome: a case report. Am J Ophthalmol Case Rep. 2022;28:101734.
4. Neustein RF, Beck AD. Circumferential trabeculotomy versus conventional angle surgery: comparing long-term surgical success and clinical outcomes in children with primary congenital glaucoma. Am J Ophthalmol 2017;183:17-24.
5. Aktas Z, Ucgul AY, Atalay HT. Outcomes of circumferential trabeculotomy and converted 180-degree traditional trabeculotomy in patients with neonatal-onset primary congenital glaucoma. J Glaucoma. 2020;29:813-818.
6. Quan AV, Chen J, Wang YE, Vanner EA, et al. Factors associated with gonioscopy-assisted transluminal trabeculotomy (GATT) complications and failure in children. Am J Ophthalmol. 2022;241:168-178.



